RESEARCH ARTICLE
Determinants of Medication Adherence and the Impact of Proactive Home Pharmacy Services in Rural South Sulawesi
Academic Editor: Indriyati Hadi Sulistyaningrum
Sciences of Pharmacy|Vol. 5, Issue 2, pp. 101-111 (2026)
CC BY 4.0-2026 Authors
Views
Downloads
Shares
Received
Nov 24, 2025Revised
Jan 19, 2026Accepted
Apr 7, 2026Published
Apr 20, 2026
Abstract
Hypertension poses a considerable health challenge in Indonesia, particularly in South Sulawesi, marked by elevated rates of medication non-adherence. Pharmacist-led home intervention models may serve as effective strategies for engaging disadvantaged populations, especially in regions with restricted healthcare access. This study seeks to investigate determinants influencing medication adherence in hypertensive patients at Puskesmas Mandai, Maros Regency, to inform the development of a pharmacist-led home care intervention model. A cross-sectional study was conducted from February to September 2025 with 35 participants, predominantly elderly women with limited educational attainment. Data were gathered through standardized questionnaires and analyzed descriptively and inferentially, incorporating forest plot visualization for odds ratios (OR). Research findings identified two primary drivers of adherence: belief in medication (OR=2.45) and information provided by pharmacists (OR=2.14). Current conditions reveal significant deficiencies 77.14% of patients lack sufficient information from pharmacists, and 51.42% do not comprehend the quality of medications utilized. These findings signify the necessity for shifting pharmaceutical services from reactive paradigms (awaiting patient visits) to proactive models (initiating patient engagement), exemplified by pharmacist-led home care, to address educational deficits and foster sustainable patient confidence. Augmenting pharmacist-led education and fostering patient trust in medicine are viable strategies to enhance adherence. These findings underscore the necessity for tailored interventions, such as home pharmacy care, to bridge knowledge gaps and strengthen pharmacists' roles in chronic disease management. Further research with larger samples is recommended to corroborate these trends.
Keywords:
Introduction
Hypertension ranks as the fourth primary cause of mortality in Indonesia. Maros Regency in South Sulawesi has 11, 428 cases, ranking it as the fourth-highest region for hypertension prevalence. Post-therapy non-adherence constitutes a significant barrier, primarily due to patients' perceptions of health, ennui, lack of ambition, or forgetfulness. In Indonesia, hypertension is identified as the fourth leading risk factor contributing to mortality, according to the Indonesian Health Survey conducted in 2023 (1). In South Sulawesi Province, specifically within Maros Regency, there exists a noteworthy prevalence of hypertension, with a recorded 11, 428 cases, positioning it as the fourth highest region for such occurrences. The occurrence of non-adherence to post-therapy treatment presents a significant challenge in this area, primarily attributed to patients' perceptions of their health status, as well as factors such as ennui, lack of motivation, or lapses in memory (2). Home care-based pharmaceutical services present a strategic approach through home visits designed to deliver education, enhance comprehension of medication, and oversee the precision of drug utilisation. This intervention is anticipated to enhance the quality of life for patients and foster adherence (3–5).
Research indicates that home pharmacy care effectively enhances medication adherence among hypertensive patients (6). This observation suggests that while Home care interventions demonstrate efficacy in behavioural dimensions, their influence on clinical outcomes warrants further investigation and analysis (7). Furthermore, the scarcity of studies concentrating on the efficacy of Home care for patients undergoing post-hypertension therapy, as well as its enduring effects on quality of life, signifies a critical research void that requires immediate attention (6–9). This study concentrates on patients undergoing therapy for post-hypertension in Maros Regency, a region characterised by a significant prevalence of cases yet lacking in robust evidence-based treatment options. This study stands out as one of the initial investigations to underscore Home care interventions within a defined geographical context and stage of care (9). The devised Home care intervention extends beyond mere education and monitoring; it incorporates a digital follow-up mechanism through text messaging platforms or phone calls, and actively engages family members as co-therapists in the realm of medication support. The amalgamation of traditional and digital methodologies enhances both the efficacy and longevity of the intervention.
Methodology
Study Design and Participants
The research methodology employed observational research, which involves the collection of quantitative data from patients. This research was conducted at the Mandai Health Center in Maros Regency from February to September 2025. A cross-sectional research design was employed, and purposive sampling procedures were utilized to select patients who met the inclusion and exclusion criteria for completing the questionnaire. The questionnaire results would be analyzed using the chi-square test and univariate analysis. The dependent variable in this study is patient medication knowledge, while the independent variable is the level of adherence to medication among hypertension patients. A compliance score below 8 is low; 8-15 is medium; and >15 is high. Subsequently, the sample study adhered to the established inclusion and exclusion criteria. This criterion encompasses patients who possess a physician's prescription, have fulfilled it at the community health center, over 18 years old, and prepared to complete the questionnaire. This criterion indicates that patients are either previously included or unable to represent the sample due to recent hypertension treatment, the presence of other complicating conditions, or pregnancy. This study utilized patient medical record data and the Medication Adherence Questionnaire (10–12). Samples were obtained from the outpatient records of patients who underwent antihypertension therapy, having received prescribed antihypertensive medicine and subsequently filled their prescriptions at the Mandai Health Center in Maros Regency, comprising a total of 35 patients. This study employed purposive sampling, wherein patients who satisfied the inclusion and exclusion criteria completed a questionnaire. A total of 35 samples were collected from the Mandai Public Health Center. The researcher will assist patients in completing the questionnaire using the Google Forms website and following the receipt of home care services. The pharmacy's home care services encompass educating patients on hypertension, emphasising medication adherence, and promoting the adoption of a healthy lifestyle following hypertension treatment (13–15).
Procedure
Data Collected and Pharmacy Home care
During the research phase, purposive sampling shall be employed to identify patients who fulfil the inclusion and exclusion criteria. They will thereafter answer a questionnaire utilising a pre-prepared drug knowledge assessment instrument. The results will then be utilised for Home care advice for patients exhibiting low adherence levels. This service will executed a minimum of twice via the POSBINDU – PTM (Integrated Post for Non-Communicable Diseases) program, and will include treatment assessment through the standard administration of 10 tablets of amlodipine 10mg. Visit data is crucial in assessing the influence of Home care services on patients' adherence to medication following hypertension treatment. This research has been approved by ethical clearance from Universitas Muslim Indonesia with recommend No. 278/A.1//KEP-UMI/V/2025.
Data Analysis
This study involved the consecutive collection of data, followed by statistical analysis utilizing the chi-square test to ascertain the relationship between independent variables (patient knowledge of their disease and administered medications) and the dependent variable (patient medication adherence level). Univariate analysis was conducted to examine associations between independent variables (knowledge level, education, pharmacist information, medication confidence) and the dependent variable (medication adherence). Additionally, simple logistic regression was performed to calculate odds ratios (OR) with 95% confidence intervals for each factor independently, quantifying the strength of association between each predictor and adherence outcomes.
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, New York, USA). Descriptive statistics were calculated to summarize demographic characteristics and questionnaire responses. One-way Analysis of Variance (ANOVA) was employed to compare mean scores across different groups (knowledge levels, adherence categories, and education levels), with statistical significance set at p < 0.05. Effect sizes (eta-squared, η²) were calculated to determine the magnitude of differences. Additionally, forest plot visualization for odds ratios (OR) with 95% confidence intervals was generated using R software, Version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria) to graphically present factors influencing medication adherence.
Results and Discussion
Patients Demography
Patients Characterized
The representative data from the 35 samples were categorised according to the demographic information of patients following hypertension treatment, specifically age, gender, education, and occupation, as illustrated in the Table 1.
| Characteristics | Category | N | Percentage (%) |
|---|---|---|---|
| Sex | Man | 13 | 37.14% |
| Woman | 22 | 62.86% | |
| Age (Years old) | < 45 | 2 | 5.71% |
| 45 – 55 | 9 | 31.43% | |
| 56 – 65 | 13 | 25.71% | |
| > 65 | 11 | 37.14% | |
| Education | Basic | 16 | 45.71% |
| Middle | 3 | 8.57% | |
| High | 8 | 22.86% | |
| Bachelor | 8 | 22.86% | |
| Occupation | Housewife | 10 | 28.57% |
| Retirement | 6 | 17.14% | |
| Civil Servant | 3 | 8.57% | |
| Businessman | 3 | 8.57% | |
| Other | 13 | 37.14% |
The questionnaire survey findings from 35 samples will yield the final numbers to evaluate the patients' knowledge level. The sample, comprising 35 individuals, was classified according to several criteria based on the patients' demographic data. Consequently, the questionnaire results indicated that the predominant respondents were female patients with an elementary school education. This aligns with the research which indicated that a greater number of female respondents experienced hypertension compared to their male counterparts, attributed to hormonal variables (reduced oestrogen levels) in women (6). The average age of the patient data exceeded 50 years, accompanied by an ambiguous understanding of hypertension. Demographic analysis revealed that patients possessed inadequate knowledge, likely attributable to their poor educational attainment, which ranged from primary to secondary levels, hindering their access to information (16). This may be due to patients' diminished confidence in consistently adhering to antihypertensive drug regimens. This occurs because individuals do not perceive the therapeutic effects directly and opt to take antihypertensive medicine solely upon experiencing symptoms, attributable to insufficient education and information provided during the dispensing of medication at the Mandai Community Health Center pharmacy (17).
Questionnaire Medication
Patients Understanding Level
Demographic analysis revealed the typical profile as female, over 50 years of age, with elementary education on the increased prevalence of hypertension in post-menopausal women. Medication adherence was moderate at 51.40%, but a significant finding was the substantial lack of lifestyle instruction offered by pharmacist, with 77.14% receiving no information. The educational deficit, exacerbated by inadequate health literacy stemming from insufficient formal education, established a cycle of poor comprehension and inconsistent drug adherence. Patients frequently ceased antihypertensive treatment when asymptomatic, indicating fundamental misunderstandings regarding chronic illness management (18, 19). Table 2 illustrates the categorisation of variable features derived from responses to the questionnaire completed by post-hypertension therapy patients at the Mandai Community Health Center during this study period. Each of these questions will reflect the patient's perception, serving as a contributing factor to elevated drug adherence.
| Variable | Category | N | Percentage (%) |
|---|---|---|---|
| Knowledge about Hypertension | Clear Knowledge | 10 | 28.57% |
| Vague Knowledge | 14 | 40.00% | |
| Without Knowledge | 11 | 31.43% | |
| Drug Price Information | Clear Knowledge | 6 | 17.14% |
| Vague Knowledge | 10 | 28.57% | |
| Without Knowledge | 19 | 54.29% | |
| Medicinal Uses Information | Exist | 32 | 91.43% |
| None | 3 | 8.57% | |
| Quality of Medication Information | Believe | 6 | 17.14% |
| Hesitate | 11 | 31.42% | |
| Not Sure | 18 | 51.42% | |
| Drug Effectiveness Information | Believe | 20 | 57.14% |
| Hesitate | 11 | 32.35% | |
| Not Sure | 4 | 11.42% | |
| Medication Regularity | Regularly Take Medication | 10 | 28.57% |
| Rarely Taking Medication | 18 | 51.42% | |
| No Medication | 7 | 20.00% | |
| Lifestyle Information | There is information | 6 | 17.14% |
| Information exists, but forgotten | 2 | 5.71% | |
| No information | 27 | 77.14% |
The significance of all facets of these questionnaire results lies in the fact that patients' comprehensive understanding of hypertension might enhance awareness of the necessity of medication adherence and increase their motivation. The accessibility of established information, including the applications and costs of medications for patients in long-term treatment, will influence the psychological and perceptual dimensions of the patients (8). Patients who comprehend the efficacy of a drug, while not perceiving its immediate effects, and the market cost of the medication they are utilising, will assess its value based on the accessibility of their treatment (20). According to recorded data, 54.30% of patients were uninformed about medicine prices, and 77.14% lacked knowledge regarding lifestyle factors, suggesting a significant information gap (20). Doubts regarding the quality and efficacy of the drug often result in the pursuit of alternative options or the cessation of the prescription entirely (21). Consequently, these qualities of the questionnaire effectively measure and elucidate the factors that contribute to inadequate medication adherence (22). The findings indicated that 7 respondents (20.00%) exhibited limited understanding, reflecting inadequate drug adherence.
The statistical test results demonstrate that patients' awareness of hypertension significantly influences adherence (Table 3), with an impact size of η² = 0.153 (big effect). The patients possessing clear knowledge (10 individuals) attained the greatest average compliance score of 15.20, whilst the cohort lacking knowledge (11 individuals) recorded the lowest score of 12.82. Despite the ANOVA test indicating no statistically significant difference (p = 0.069), the clinical pattern observed was notably consistent. The principal discovery arose from the examination of medication adherence levels. The findings indicate a statistically significant difference (F = 12.91; p < 0.001) among the three groups, accompanied by a substantial effect size (η² = 0.446). The cohort that consistently administered medicine (n=10) achieved the greatest mean score (15.00), succeeded by the cohort that intermittently utilized medication (n=18) with a score of 13.50, and the cohort that abstained from medication (n=7) with the lowest score (11.00). This distinct gradient indicates that medication adherence is not merely a result, but a crucial predictive element in the comprehensive management of hypertension. Despite the knowledge level exhibiting a favorable trend (η² = 0.153, strong effect), it has not yet attained statistical significance (p = 0.069). The group possessing clear knowledge (n=10) achieved an average score of 15.20, whereas the group lacking information (n=11) attained just 12.82. These results suggest that knowledge constitutes a crucial basis, although does not inherently ensure compliance in the absence of additional supporting elements.
| Variable Factor | Group | n | Mean Score | F | η2 (Eta²) | p-value | Significant |
|---|---|---|---|---|---|---|---|
| Knowledge Level | Clear | 10 | 15.20 | 2.89 | 0.153 | 0.069 | Not |
| Unclear | 14 | 13.71 | |||||
| Did not have | 11 | 12.82 | |||||
| Adherence Level | Regularly | 10 | 15.00 | 12.91 | 0.446 | < 0.001 | Significant |
| Rarely | 18 | 13.50 | |||||
| No medication | 7 | 11.00 | |||||
| Education Level | Elementary School | 16 | 13.38 | 0.68 | 0.062 | 0.569 | Not |
| Junior High School | 3 | 14.33 | |||||
| High School | 8 | 13.63 | |||||
| Bachelor or Higher | 8 | 14.63 | |||||
| Note: Knowledge: η2η2 = 0.153 (Big Effect); Adherence: η2η2 = 0.446 (Big Effect); Education: η2η2 = 0.062 (Medium Effect) | |||||||
The variable of formal education, with η² = 0.062 (medium effect), indicates that patients with higher educational attainment exhibit superior compliance scores in comparison to those who are elementary school graduates. While statistical significance has not yet been attained, potentially due to the limited sample size, the clinical implications of these three factors are substantial and pertinent. The data unequivocally suggests that any intervention aimed at enhancing adherence, such as pharmacist-led home care, must incorporate health education components customized to the patient's literacy level and strategies for empowerment rooted in family and community to attain optimal and sustainable outcomes.
The questionnaire data collected from outpatient hypertension therapy patients at Mandai Public Health Center were evaluated using the chi-square test to investigate the relationship between knowledge and medication adherence patterns in post-hypertension therapy patients.
| Adherence | Odds Ratio | CI 95% (Lower- Upper) | (p-value) |
|---|---|---|---|
| Compliance | 0.198 | 0.073 -0.531 | < 0.001 |
| Non-Compliance | 3.407 | 1.016 – 0.531 |
An analysis was conducted at the Mandai Public Health Center to determine the relationship between patients' knowledge and their adherence to medicine after hypertension therapy (Table 4). The chi-square test yielded a p-value less than 0.05, suggesting a significant influence. The statistics show that the level of adherence is much lower than expected due of the high influence of lack of knowledge on the level of adherence (OR = 3.407, CI 1.016-11.432). Consequently, medication adherence is significantly impacted by having adequate information. The outcome is in line with earlier studies on the level of adherence to taking antihypertensive medicine, where the p-value was less than 0.05. The results showed that hypertension patients' adherence to taking antihypertensive medication increased as their level of knowledge increased (16, 21).
There are 7 individuals (20.00%) with low adherence levels in this feature; they fall into two categories: those with imprecise understanding of hypertension and those without clear knowledge of the condition. Next, 10 persons (28.00%) with hazy understanding and 6 people (17.00%) with unclear knowledge are found at intermediate adherence levels. A person's health-related attitudes and beliefs are shaped by their decision-making process, which in turn determines their level of adherence. A patient's conviction in consistently following the requirements for medication adherence might be influenced by their amount of knowledge about their ailment, according to this data and statistical analysis. Medication adherence is positively correlated with patients' level of sickness knowledge.
The results of the questionnaire showed that 77.14% of patients who got medication from the pharmacy did not receive this information, and that the only drug information given to patients was the dosage and the medication's intended use, according to the information services offered at the Mandai Community Health Center. The results show that people's knowledge affects their degree of compliance. Patients are less likely to remember to take their medications as prescribed because healthcare providers, especially pharmacist, do not provide enough information on treatment. This research reveals that the health center pharmacy is understaffed and underperforming in its job as a result of the large number of people requiring medication following medical exams (18, 24). So, they can't give comprehensive medication information services because of space and time constraints. Patients' ideas and attitudes about medication adherence shall be impacted. Patients with poor scores and non-adherence to medication intake based on the medication adherence questionnaire are educated and monitored through home care services offered at the Mandai Community Health Center. According to the data that was collected, patients do not stick to their treatment plans because they do not have enough knowledge due to a lack of education. As part of the home care service, patients receive education in the comfort of their own home. After that, they are asked to fill out a questionnaire that will help determine how much of an improvement there was in their compliance levels after receiving home care. The researcher, along with healthcare professionals from the Mandai Community Health Center, visited the pharmacy to observe their home care service as part of this study. Patients with low scores, specifically 9, from the prior questionnaire continued to get services for re-evaluation. Seven patients reported not taking their prescription, had moderate understanding, and had pretest scores below average (25, 26).
The pharmacist role in this study was to visit patients' homes as part of Home care services, where they educated patients about the importance of taking their medications as prescribed and shared information about healthy lifestyle changes that hypertension patients could make to improve their quality of life (27, 28). Following the teaching session, patients were given opportunity to return and fill out a post-questionnaire regarding their medication adherence levels. This was followed by a brief interview with the researcher. As illustrated in Figure 1, the forest plot demonstrates the relationship between patient characteristics and adherence to hypertension treatment.
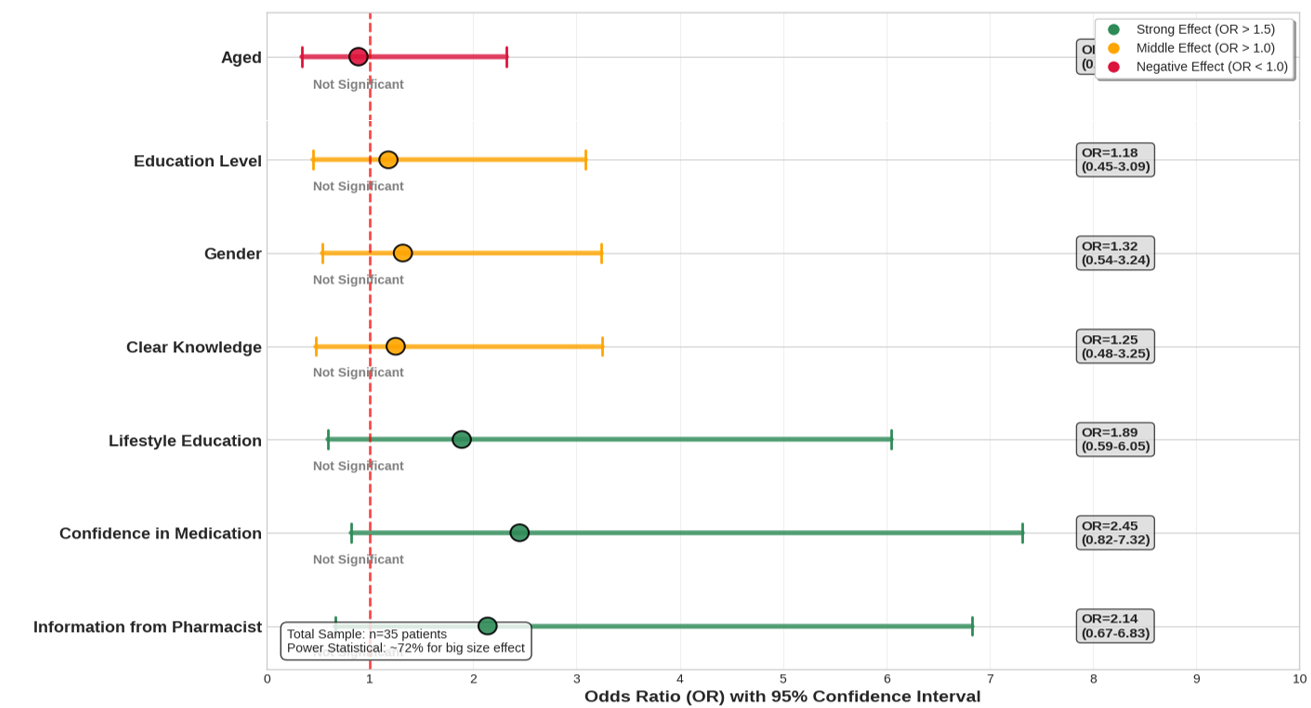
The forest plot indicates while no component reached statistical significance, a clinical trend was seen. The belief in the medication had the significant impact, with an odds ratio (OR) of 2.45, succeeded by information from pharmacist (OR 2.14) and lifestyle education (OR 1.89). This suggests patients who have confidence in their medication's efficacy, receive information from pharmacist, and comprehend the significance of a healthy lifestyle are more inclined to comply with hypertension therapy (7, 13). Demographic characteristics, including female gender, advanced education, and knowledge level, exhibit a diminished impact, however being above 55 years of age negatively affects adherence. This pattern indicates that psychosocial and informational determinants may play a more influential role than demographic variables in predicting adherence outcomes. The results underscore the necessity for treatments aimed at enhancing patient trust and improving pharmacist education, but larger sample studies are required to validate these findings (29, 30).
Univariate Analysis for Intervention Pharmacy Home care
Subsequent to the intervention, a statistically significant enhancement in the post-test scores was seen. The results exhibit a considerable divergence from the pre-test regarding both knowledge and medication adherence. This aligns with previous research that identified a statistically significant change between pre- and post-test adherence levels (31, 32). Consequently, patients' physical and environmental health may enhance due to a transformation in their perceptions of therapy, which subsequently encourages them to modify their lifestyle and comply more rigorously with their treatment regimens.
| Variabel Research | 95% Confident Interval | Mean | p-value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Knowledge Level | 0.503 | 1.497 | 0.229 | < 0.001* |
| Drug Price | 0.456 | 1.354 | 0.152 | 0.003* |
| Medicinal Uses | 1.346 | 1.987 | 0.181 | < 0.001* |
| Quality of Medication | 0.456 | 1.354 | 0.152 | 0.003* |
| Drug efficacy | 0.800 | 1.962 | 0.381 | 0.635 |
| Medication Regularity | 0.048 | 1.000 | 0.952 | < 0.001* |
| Lifestyle Information | 0.280 | 0.862 | 1.343 | < 0.001* |
| Note: * is significant | ||||
The statistical analysis results, utilising the Univariate test shown in Table 5, indicate that a knowledge level of < 0.001 significantly influences and enhances clinical outcomes following educational intervention via Home care services. The greater the knowledge, the superior the clinical outcomes attained. When patients successfully adopt and maintain a healthy lifestyle, it illustrates how the quality of education has effectively influenced changes in their behaviour (29).
The patient's comprehension of the quality and information concerning drug prices significantly (p-value < 0.05) suggests an inclination to enhance patient motivation for consistent medication adherence, as trust in the medication is crucial for patients' perception that the drugs they use originate from a credible source, particularly since many patients frequently perceive generic drugs as potentially inferior in quality. This occurs due to the belief that a clear understanding of a drug's price can signify its quality, leading patients, particularly those with limited financial resources, to feel compelled to adhere to prescribed medications, thereby necessitating transparency in drug pricing and availability. Nonetheless, there was no impact on efficacy, potentially due to patients' unfamiliarity and lack of comprehension regarding therapeutic effectiveness (13).
The provision of drug information services via Home care by pharmacy workers significantly enhances patient adherence. The conditions at the community health clinic where the research was conducted remain unsatisfactory, and there is a deficiency of pharmacy personnel, indicating a need for additional enhancement in this area. The involvement of healthcare professionals is essential in the management of hypertensive patients, including the provision of education regarding hypertension. By elucidating the utility, quality, efficacy, and significance of adhering to a regular drug regimen, it constitutes novel knowledge. To enhance patient adherence, effective communication and education from healthcare professionals are essential to consistently promote compliance with antihypertensive medication, hence improving quality of life (33, 34).
Discussion
The analysis of questionnaire data from all respondents indicates the intricate challenges associated with adherence to hypertension therapy within the community. The demographic profile indicates a predominance of women, with a significant portion possessing basic education, and and a substantial representation of the senior population, which is epidemiologically recognised as a vulnerable category for non-adherence to chronic therapy. Data indicates that patients' comprehension of hypertension remains significantly inadequate, with merely possessing a clear grasp, exhibiting ambiguous knowledge, and without any knowledge whatsoever. This condition is associated with a compliance pattern in which of patients adhere to their prescription regimen, while we have compliance challenges, including who frequently forget to take their medication. The identified pivotal element is the inadequate involvement of pharmacist in delivering education and information to patients. The 51.42% of patients reported insufficient information on their quality of drugs, while 77.14% did not receive lifestyle education from the pharmacist. This engenders a knowledge deficit that results in misunderstandings regarding hypertension management, with numerous patients initiating medication solely in the presence of symptoms and discontinuing treatment upon feeling well. Statistical study, albeit not significant (p > 0.05), indicates a persistent tendency whereby individuals with superior knowledge generally exhibit greater adherence scores (35–37).
The deployment of pharmacy Home care provides a strategic strategy to overcome the educational restrictions present during typical healthcare facility visits. Home care enables pharmacist to perform a thorough evaluation of patients' prescription adherence patterns, comprehension of their conditions, obstacles to compliance, and environmental influences (32). Home interventions facilitate a tailored approach that takes into account the patient's unique circumstances, including their educational background, familial support, and daily routines. Pharmacists might recognise practical issues such as challenges in accessing pharmaceutical packaging, conflicting medication schedules with activities, or inadequate medication storage (38, 39).
The discovery that 51.42% of patients lacked comprehension of the quality of their prescriptions and that 54.3% were unaware of drug pricing (p = 0.003) necessitates meticulous interpretation within the Indonesian context. At Puskesmas Mandai, the majority of antihypertensive medications are dispensed under the JKN national health insurance program, incurring little or minimal out-of-pocket expenses for patients. Consequently, the 'price worry' articulated by patients likely signifies perceived value rather than genuine financial hardship. Patients may associate higher-priced prescriptions with superior quality, resulting in doubt regarding the efficacy of subsidized or generic treatments. This image is vital as generic medications are frequently distributed at Indonesian public health facilities. Patients lacking knowledge about drug price may erroneously perceive generic pharmaceuticals as inferior to branded products, hence diminishing their trust in medication efficacy, which we identified as the most significant predictor of adherence (OR = 2.45). We have amended the conversation to directly link price information to trust in the quality of generics, highlighting that pharmacist education must rectify this misperception by elucidating bioequivalence and the stringent clearance process for generic pharmaceuticals in Indonesia.
Moreover, pharmacy Home care promotes a family center model, enabling pharmacists to engage family members as advocates for adherence. In the Indonesian context, which places significant emphasis on family, this strategy possesses considerable potential for efficacy. Families can act as reminders for pharmaceutical regimens, assist in monitoring side effects, and facilitate lifestyle modifications. Home care enables pharmacist to directly evaluate eating habits and physical activity (40–42). The execution of pharmacy Home care encounters structural obstacles, including the substantial workload of pharmacists in healthcare settings, constrained resources, and the absence of a definitive finance framework for Home care services. A collaborative framework involving community health workers and Posbindu cadres is essential for ensuring the sustainability of this intervention (38, 43). Moreover, the incorporation of technology via telemonitoring and remote counselling might enhance service coverage without straining current resources. This research underscores the necessity of redefining pharmacist' roles from simple presenters to educators and collaborators in chronic disease treatment. Home pharmacy care serves not only as a method to enhance adherence but also as a sustainable investment in fostering patients' autonomy in health management. The successful execution necessitates governmental endorsement, a reconfiguration of pharmacy education, and a unified commitment from all stakeholders to realise patient-centered pharmaceutical services.
There are some problems with this study that need to be pointed out. First, while adherence and knowledge exhibited substantial effect sizes, knowledge and education failed to reach statistical significance. The study was likely underpowered to detect significant differences in demographic variables, as indicated by the contrast between substantial effect sizes and non-significant p-values. Even though the odds ratios were clinically significant, the forest plot didn't show any factors that were statistically significant because the sample size was too small (n = 35). To confirm these patterns, larger sample sizes are necessary in subsequent research. Second, causal relationships cannot be inferred due to the study's cross-sectional observational design lacking a control group. The identified correlations do not reflect intervention effects; instead, they represent baseline correlations. Third, the single-center design of one community health center limits generalizability to various Indonesian contexts.
Conclusion
The results of this study indicate the role of pharmacy in improving medication adherence in post-therapy hypertensive patients at the Mandai Community Health Center with Home care pharmacy services are proving to be very effective in improving medication adherence because they offer more privacy. Statistical study, indicates a persistent tendency whereby enhanced knowledge correlates with increased adherence. Home pharmacy care emerges as a strategic solution to deliver a personalised approach, engage families, and directly tackle adherence barriers within the patient's home environment, while simultaneously bridging the information gap that has been a critical issue in the health care medical service of chronic hypertension and supporting sustainable behavioural changes that contribute to improved treatment outcomes.
Declarations
Acknowledgment
Thank you to Universitas Muslim Indonesia and Mandai Health Centre for supporting this research. Thanks to QuillBot.ai Premium for help me adjust grammar in this article.
Conflict of Interest
The authors declare no conflicting interest.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to confidentiality agreements with participating institutions and privacy considerations of patient data. However, anonymized data may be made available from the corresponding author upon reasonable request and with permission from the relevant ethics committee
Ethics Statement
This study has gone through an ethical review from the Health Research Ethics Commission of Universitas Muslim Indonesia with the number 278/A.1/KEP-UMI/V/2025 on registered UMI012503276 May 20, 2025.
Funding Information
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
References
- Nakanishi M, Mizuno T, Mizokami F, Koseki T, Takahashi K, Tsuboi N, et al. Impact of pharmacist intervention for blood pressure control in patients with chronic kidney disease: A meta‐analysis of randomized clinical trials. J Clin Pharm Ther. 2020;46(1):114-120. doi: https://doi.org/10.1111/jcpt.13262
- Maulana Kamri A, Kosman R, Rahayu D. Analisis efektivitas biaya penggunaan amlodipin dibandingkan kaptopril pada pasien hipertensi di rumah sakit umum daerah majene periode januari hingga juni tahun 2019. Jiis. 2021;6(2):262-271. doi: https://doi.org/10.36387/jiis.v6i2.718
- Füri J, Widmer A, Bornand D, Berger C, Huttner B, Bielicki JA. The potential negative impact of antibiotic pack on antibiotic stewardship in primary care in Switzerland: a modelling study. Antimicrob Resist Infect Control. 2020;9(1):60. doi: https://doi.org/10.1186/s13756-020-00724-7
- Kamri AM, Kosman R, Pujawanti A, Ananda R, Ferawati S, Asnawi N, et al. Pharmacists in antibiotic resistance prevention education at Makassar Mandai Market. ABDIMAS J. Pengabdi. Masy. Univ. Merdeka Malang. 2023;8(1):72-81. doi: https://doi.org/10.26905/abdimas.v1i1.8971
- Boehmer K, Johnson C. A Pilot Project to Implement a Pharmacist-Managed Remote Blood Pressure Monitoring Service. Journal of Pharmacy Practice. 2024;38(3):294-298. doi: https://doi.org/10.1177/08971900241285943
- Kawana M. The Effect of Clinical Research by Community Pharmacists on the Medical Field —The Perspective of Scientists in the Community Can Improve a Patient's Circumstances. Yakugaku Zasshi. 2022;142(3):219-224. doi: https://doi.org/10.1248/yakushi.21-00174-4
- Dopp JM, Lange A, Maursetter L. Interdisciplinary Telehealth Team Positively Impacts Difficult-to-Control Hypertension in CKD. Kidney360. 2023;4(6):e817-e823. doi: https://doi.org/10.34067/kid.0000000000000130
- Naqvi IA, Strobino K, Kuen Cheung Y, Li H, Schmitt K, Ferrara S, et al. Telehealth After Stroke Care Pilot Randomized Trial of Home Blood Pressure Telemonitoring in an Underserved Setting. Stroke. 2022;53(12):3538-3547. doi: https://doi.org/10.1161/strokeaha.122.041020
- Agnol RD, dos Santos MT, Michalowski MB, Einsfeld L. Pharmacists’ interventions on 2 years of drug monitoring in an oncology pediatric inpatient ward. J Oncol Pharm Pract. 2021;28(8):1754-1762. doi: https://doi.org/10.1177/10781552211041037
- Andi Maulana K, Ira A. Knowledge influence in the compliance rate of taking drugs tuberculosis. Pharmacoscript. 2023;6(2):208-218. doi: https://doi.org/10.36423/pharmacoscript.v6i2.1285
- Nair D, Green JA, Marra CA. Pharmacists of the future: What determines graduates’ desire to engage in patient-centred services?. Research in Social and Administrative Pharmacy. 2021;17(3):545-552. doi: https://doi.org/10.1016/j.sapharm.2020.04.030
- Lau D, Ringrose J, McAlister FA, Fradette M, Wood PW, Boulanger P, et al. Telemonitoring and protocolized case management for hypertensive community dwelling older adults (TECHNOMED): a randomized controlled trial. Journal of Hypertension. 2022;40(9):1702-1712. doi: https://doi.org/10.1097/hjh.0000000000003202
- Chen YT, Yeh WY, Hu YC, Yang SM, Pan RH, Chen TH, et al. Effectiveness of a nationwide community pharmacist-led program promoting home blood pressure monitoring on hypertension control and self-management. Hypertens Res. 2025;49(2):315-327. doi: https://doi.org/10.1038/s41440-025-02422-6
- Malik M, Hussain A, Aslam U, Hashmi A, Vaismoradi M, Hayat K, et al. Effectiveness of Community Pharmacy Diabetes and Hypertension Care Program: An Unexplored Opportunity for Community Pharmacists in Pakistan. Front. Pharmacol. 2022;13:710617.doi: https://doi.org/10.3389/fphar.2022.710617
- McKeirnan KC, Frazier K, Kherghehpoush S, Sedaghat E. Using the patient activation measure during a pharmacist-led rural patient home visit pilot project. Journal of the American Pharmacists Association. 2021;61(4):e279-e283. doi: https://doi.org/10.1016/j.japh.2021.01.005
- Van Prooyen AM, Hicks JL, Lin E, Davis SS, Singh A, Harris DA, et al. Evaluation of An Inpatient Pharmacy Consult on Discharge Medications in Bariatric Surgery Patients. Journal of Pharmacy Practice. 2021;36(2):203-212. doi: https://doi.org/10.1177/08971900211030238
- Vordenberg SE, Kim J, Serlin DC, Fan AL, Choe HM. Pharmacist engagement in a community pharmacy hypertension management program in collaboration with an academic medical center. American Journal of Health-System Pharmacy. 2022;79(13):1110-1114. doi: https://doi.org/10.1093/ajhp/zxac081
- Commodore-Mensah Y, Chen Y, Ogungbe O, Liu X, Metlock FE, Carson KA, et al. Design and rationale of the cardiometabolic health program linked with community health workers and mobile health telemonitoring to reduce health disparities (LINKED-HEARTS) program. American Heart Journal. 2024;275:9-20. doi: https://doi.org/10.1016/j.ahj.2024.05.008
- Margolis K, Bergdall A, Crain AL, JaKa M, Anderson J, Solberg L, et al. Comparing Telehealth and Clinic-Based Care for Lowering Uncontrolled High Blood Pressure. Patient-Centered Outcomes Research Institute (PCORI). 2023;. doi: https://doi.org/10.25302/03.2023.ihs.150731146
- Lynton JJ, Mersch A, Ferguson PJ. Multidisciplinary practice advancement: Role of a clinical pharmacy specialist in a pediatric specialty clinic. American Journal of Health-System Pharmacy. 2020;77(21):1771-1777. doi: https://doi.org/10.1093/ajhp/zxaa246
- Gavrilova A, Bandere D, Logviss K, Šmits D, Urtāne I. Adherence Level to Arterial Hypertension Treatment: A Cross-Sectional Patient Survey and Retrospective Analysis of the NHS Prescription Database. Healthcare. 2021;9(8):1085. doi: https://doi.org/10.3390/healthcare9081085
- Craig KJT, Zaleski AL, MacKenzie SM, Butler BL, Youngerman RA, McNutt SL, et al. Pharmacoinformatics-enabled Interventions Improved Care Coordination and Identified Pharmacy-Related Safety Issues in a Multicultural Medicare Population. Appl Clin Inform. 2024;15(02):320-326. doi: https://doi.org/10.1055/a-2297-4334
- 23. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale (NJ): Lawrence Erlbaum Associates; 1988. 567 p.
- Shaw RJ, Montgomery K, Fiander C, Bullock K, Craig R, Pennington G, et al. Mobile Monitoring-Enabled Telehealth for Patients with Complex Chronic Illnesses: IOS Press; 2024. doi: https://doi.org/10.3233/shti230954
- Masnah C, Daryono D, Subakir S. Edukasi Mandiri dalam Upaya Peningkatan Kepatuhan Berobat Penderita Hipertensi di Kota Jambi. Creat J. Cumn Enga. 2024;7(11):5042-5060. doi: https://doi.org/10.33024/jkpm.v7i11.17431
- Rghebi N, Elmzughi R, Alrgaei R, Belal M. Knowledge, Attitudes, and Practices of Libyan Community Pharmacists Towards Vitamin Supplements: A Cross-Sectional Study. sciphar. 2025;4(1):9-19. doi: https://doi.org/10.58920/sciphar0401303
- Mertz A, Fair C, Pol J. Geriatric Pharmacotherapy Case Series: Clotting and Gender-Affirming Care. sr care pharm. 2024;39(9):319-324. doi: https://doi.org/10.4140/tcp.n.2024.319
- Rizvi-Toner A, Coe AB, Friese CR, Manojlovich M, Wallner L, Farris KB. Patient symptoms, self-management, and unscheduled healthcare use during the first 6 months of targeted oral anticancer agent therapy: protocol for a mixed-methods US study. BMJ Open. 2024;14(2):e081375. doi: https://doi.org/10.1136/bmjopen-2023-081375
- Lin YW, Chen PC, Lin CH, Lin MH. Investigating medication adherence among Taiwanese patient with hypertension, hyperlipidemia, and diabetes: A pilot study using the Chinese version of a Two-Part Medication Nonadherence Scale and the NHI MediCloud system. PLoS ONE. 2024;19(7):e0304442. doi: https://doi.org/10.1371/journal.pone.0304442
- Gastens V, Kiszio B, Del Giovane C, Tsuyuki R, Paradis G, Chiolero A, et al. Pharmacist interventions to improve hypertension management: protocol for a systematic review of randomised controlled trials. BMJ Open. 2022;12(5):e059399. doi: https://doi.org/10.1136/bmjopen-2021-059399
- Ben Mabrouk A, Larbi Ammari F, Werdani A, Jemmali N, Chelli J, Mrabet HE, et al. Parental self-medication with antibiotics in a Tunisian pediatric center. Therapies. 2022;77(4):477-485. doi: https://doi.org/10.1016/j.therap.2021.10.007
- Bosworth HB, Patel UD, Lewinski AA, Davenport CA, Pendergast J, Oakes M, et al. Clinical Outcomes Among High-Risk Primary Care Patients With Diabetic Kidney Disease. Medical Care. 2024;62(10):660-666. doi: https://doi.org/10.1097/mlr.0000000000002043
- Fiscella KA, Sass E, Sridhar SB, Maguire JA, Lashway K, Wong G, et al. Team-based home blood pressure monitoring for blood pressure equity a protocol for a stepped wedge cluster randomized trial. Contemporary Clinical Trials. 2023;134:107332. doi: https://doi.org/10.1016/j.cct.2023.107332
- Vordenberg SE, Thompson AN, Vereecke A, Smrke R, Serlin DC, Fan AL, et al. Primary care provider perceptions of an integrated community pharmacy hypertension management program. Journal of the American Pharmacists Association. 2021;61(3):e107-e113. doi: https://doi.org/10.1016/j.japh.2020.11.022
- Wells C, Warren AC, Scott MA. Development and implementation of ambulatory care pharmacy services at an internal medicine clinic. American Journal of Health-System Pharmacy. 2024;81(17):e528-e534. doi: https://doi.org/10.1093/ajhp/zxae102
- Good M, Hoskins R, Lund BC, Ten Eyck P, Dixon B, Cohen J, et al. A clinical trial evaluating pharmacist-guided self-management of hypertension among veterans with CKD, rationale and study design. Contemporary Clinical Trials. 2025;154:107950. doi: https://doi.org/10.1016/j.cct.2025.107950
- Yasin NM, Kurniawati F, Ridhayani F. Bridging gaps in medication therapy management at community health centers: A mixed-methods study on patient perceptions and pharmacists' preparedness. Exploratory Research in Clinical and Social Pharmacy. 2025;17:100554. doi: https://doi.org/10.1016/j.rcsop.2024.100554
- Ishak AM, Mukamal KJ, Wood JM, Vyavahare M, Cluett JL, Juraschek SP. Pharmacist‐led rapid medication titration for hypertension management by telehealth: A quality improvement initiative. J of Clinical Hypertension. 2024;26(2):217-220. doi: https://doi.org/10.1111/jch.14750
- Gastens V, Tancredi S, Kiszio B, Del Giovane C, Tsuyuki RT, Paradis G, et al. Pharmacists delivering hypertension care services: a systematic review and meta-analysis of randomized controlled trials. Front. Cardiovasc. Med. 2025;12. doi: https://doi.org/10.3389/fcvm.2025.1477729
- Harnett A, Sahm LJ, Burke E, Lyons D, Byrne S. Application of a screening tool to understand the medication habits of patients with swallowing difficulty: a prospective observational study. Int J Clin Pharm. 2025;47(5):1224-1231. doi: https://doi.org/10.1007/s11096-025-01901-7
- Chaudhri K, Liu H, Rodgers A, Day R, Atkins ER, Gnanenthiran SR. Patients' and providers' perspectives of a dose administration aid strategy to improve cardiovascular disease prevention in Australian primary healthcare. BMC Health Serv Res. 2025;25(1). doi: https://doi.org/10.1186/s12913-025-12391-8
- Okpala M, Izeogu C, Wang M, Green C, Cooksey G, Nguyen T, et al. Video-based Intervention to Reduce Treatment and Outcome Disparities in Adults Living with Stroke or Transient Ischemic Attack (VIRTUAL): protocol for a randomized controlled trial. Trials. 2025;26(1). doi: https://doi.org/10.1186/s13063-025-09003-5
- Srimongkhol P, Anutrakulchai S, Theeranut A, Methakanjanasak N, Lertsinudom S. Development of Chronic Kidney Disease Screening Integrative Care Model Led by Community Pharmacists. Pharmacy. 2025;13(1):27. doi: https://doi.org/10.3390/pharmacy13010027