RESEARCH ARTICLE
Impact of Hormonal Therapy Regimens and Adverse Drug Reactions on Quality of Life in Breast Cancer Patients at Dr. Moewardi Regional General Hospital, Surakarta
Sciences of Pharmacy|Vol. 5, Issue 2, pp. 176-188 (2026)
CC BY 4.0-2026 Authors
Views
Downloads
Shares
Received
Jan 19, 2026Revised
Mar 27, 2026Accepted
May 11, 2026Published
May 19, 2026
Abstract
Breast cancer remains the most common malignancy among women worldwide, and hormonal therapy is a cornerstone in the management of hormone receptor-positive cases, although its impact on adverse drug reactions (ADRs) and quality of life (QoL) remains a concern. This study aimed to evaluate the association between hormonal therapy patterns, ADRs, and QoL in breast cancer patients. An observational analytic study with a crosssectional design was conducted at Dr. Moewardi Regional General Hospital, Surakarta, from January to June 2025, involving 64 patients selected through consecutive sampling. Data were collected from medical records and structured interviews. QoL was assessed using the EORTC QLQ-C30 questionnaire, and ADRs were evaluated using the FACT-ES instrument. Bivariate and multivariate logistic regression analyses were performed. Most patients were aged < 50 years (60.9%) and diagnosed at an advanced stage (57.8%). No significant associations were found between sociodemographic or clinical characteristics and type of therapy, survival duration, or ADR severity (all p> 0.05). The most common ADRs were fatigue (51.6%) and hot flushes (50%). QoL assessment showed good functional status (mean = 79.65) and low symptom burden (mean = 25.06), but poor global health status (mean = 26.30). Cancer stage (p = 0.010) and type of therapy (p = 0.027) were significantly associated with QoL. Multivariate analysis confirmed that advanced-stage cancer (OR = 0.31; 95% CI: 0.14-0.68; p = 0.004) and combination therapy (OR = 0.44; 95% CI: 0.21-0.92; p = 0.024) were independent predictors of poorer QoL. These findings highlight the importance of individualized treatment strategies to optimize patient quality of life.
Introduction
Breast cancer is the most commonly diagnosed malignancy among women worldwide and remains a significant public health concern. Globally, improvements in early detection and advances in therapy have substantially increased survival rates. Data from the World Health Organization indicate that mortality rates in high-income countries have declined over recent decades, leading to a growing population of breast cancer survivors (1, 2). In Indonesia, breast cancer is the most prevalent cancer among women, with a continuously increasing incidence trend. Based on Global Cancer Observatory (GLOBOCAN) data from 2020, the incidence of breast cancer in Indonesia reached approximately 42.1 cases per 100,000 women, with a mortality rate of 16.6 per 100,000 women. Previous data reported an incidence of around 37.4 per 100,000 population in 2019, reflecting a consistent rise in cases. This increasing burden has led to a greater need for long-term survivorship care (3).
Approximately 70% of breast cancer cases are hormone receptor-positive, making endocrine therapy a key component of treatment. Adjuvant Hormone Therapy (AHT), including aromatase inhibitors and selective estrogen receptor modulators such as tamoxifen, has been shown to reduce the risk of recurrence by up to 40% and mortality by about one-third (4, 5). However, long-term use for 5-10 years increases the risk of chronic side effects that may negatively impact patients’ quality of life (6). Previous studies have reported that symptoms such as fatigue, musculoskeletal pain, and vasomotor symptoms are among the most commonly experienced adverse effects, with prevalence varying but reaching over 50% in some patient populations (7-9).
From the early stages of the disease trajectory, the quality of life of breast cancer survivors is influenced by both clinical and non-clinical factors. Clinical factors such as disease stage and type of therapy have been associated with quality-of-life outcomes, with patients at advanced stages and those receiving combination therapy generally experiencing poorer quality of life compared to those at early stages or receiving single therapy (10, 11). In addition, non-clinical variables such as treatment adherence, comorbidities, and socioeconomic status play a critical role in determining quality of life and may act as confounding variables in the relationship between treatment and patient outcomes (9, 12). However, these factors are often not included simultaneously in analytical models in previous studies.
Despite the growing body of research on quality of life among breast cancer survivors, several specific and measurable research gaps remain. First, most previous studies have only examined one or two variables separately, without conducting multivariable analyses that integrate disease stage, type of therapy, and key confounders into a comprehensive model (12). Second, many studies have not systematically applied patient-reported outcomes (PROs), resulting in suboptimal measurement of the subjective aspects of patients’ quality of life (13, 14). Third, in Indonesia, research on the quality of life of breast cancer survivors remains limited and is generally descriptive in nature, with few studies quantitatively examining the relationship between key clinical factors and quality of life while controlling for important confounders such as adherence, comorbidities, and socioeconomic status (3, 14). Consequently, robust evidence regarding the independent determinants of quality of life in this population is still lacking.
Furthermore, the survivorship phase also influences patients’ adaptation to the disease and its treatment. Survivorship is commonly categorized into re-entry, short-term, and longterm phases, each associated with distinct physical and psychological challenges (15, 16). However, these phase variations are often not systematically analyzed in relation to quality of life.
Based on these gaps, this study aims to evaluate factors associated with quality of life among breast cancer survivors undergoing hormonal therapy. Specifically, this study tests the following hypotheses: (1) cancer stage and type of therapy (combination chemotherapy and hormonal therapy versus hormonal therapy alone) are significantly associated with quality of life; and (2) after controlling for confounding variables (age, menopausal status, HER2 status, duration of therapy, and other relevant clinical factors), advanced stage and combination therapy are independent predictors of poorer quality of life. This study is expected to provide more comprehensive and integrated empirical evidence on the determinants of quality of life among breast cancer survivors in the Indonesian context and to support the development of more patient-centered survivorship care strategies.
Methodology
Study Design and Research Subjects
This study employed an observational analytic design with a cross-sectional approach conducted at the outpatient and inpatient units of Dr. Moewardi Regional General Hospital, Surakarta, from January to June 2025. The cross-sectional design was selected to evaluate the association between hormonal therapy patterns, adverse drug reactions (ADRs), and quality of life at a single point in time. Subjects were selected using consecutive sampling, including all eligible patients during the study period. The sample size was determined based on feasibility and the total number of eligible patients attending the study site during the study period.
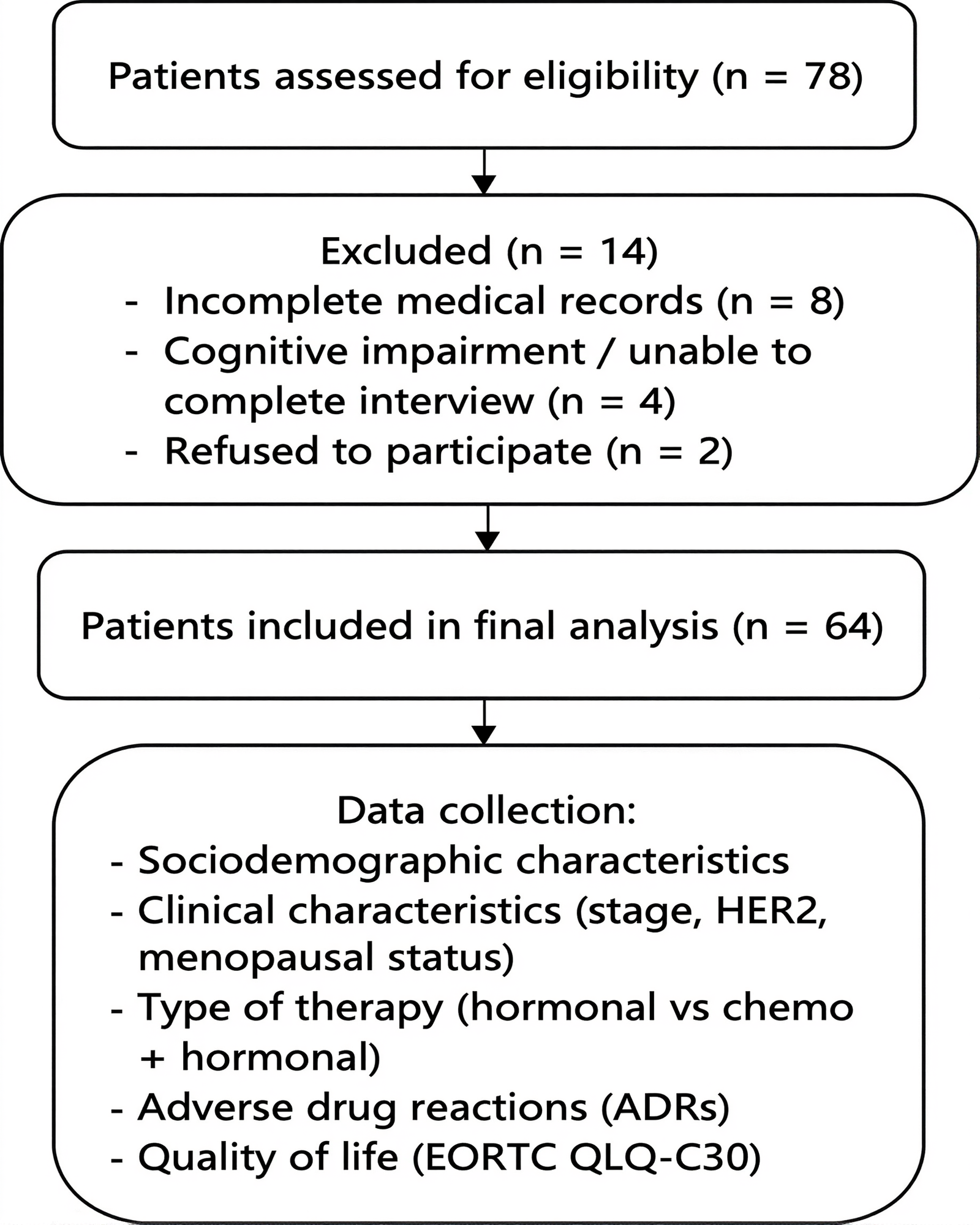
Although a formal sample size calculation was not performed, this is acknowledged as a limitation of the study. Inclusion criteria were female patients aged ≥18 years, diagnosed with breast cancer confirmed by medical records, hormone receptorpositive (estrogen receptor [ER] and/or progesterone receptor [PR] positive), known HER2 status (positive or negative), receiving hormonal therapy (tamoxifen and/or aromatase inhibitors), either as monotherapy or in combination with chemotherapy, and willing to participate with written informed consent. Exclusion criteria included central nervous system metastasis, severe comorbidities, cognitive impairment, multiple malignancies, or pregnancy. A total of 78 patients were screened, and 14 were excluded due to incomplete medical records (n = 8), cognitive impairment or inability to complete interviews (n = 4), and refusal to participate (n = 2) (Figure 1). Therefore, 64 patients were included in the final analysis.
Administrative and Ethical Approval
This study received ethical approval from the Health Research Ethics Committee of Dr. Moewardi Hospital, Surakarta, under approval number 1.287/VI/HREC/2025. All participants were provided with a clear explanation of the study objectives, procedures, potential risks, and benefits prior to enrollment. Written informed consent was obtained from all participants before data collection.
Data Source
Data collection integrated medical record reviews and structured interview. The Quality of Life (QoL) using the Indonesian version of EORTC QLQ-C30 questionnaire, validated by Perwitasari et al. (2011) (17), and the questionnaire used to assess ADRs in this study was the Functional Assessment of Cancer Therapy-Endocrine Symptoms (FACT-ES), adapted from the study by Fallowfield et al. (1999) (18), The Indonesian version of FACT-ES was used following linguistic adaptation. However, internal consistency reliability was not retested in this study, which is acknowledged as a limitation. Clinical data included disease stage, status HER2, treatment type, and duration.
Quality of Life (QoL), Quality of life assessment covered global health status, functional scales (physical, role, emotional, cognitive, social), and symptom scales (fatigue, pain, nausea/vomiting). Questionnaire administration followed standardized protocols to minimize interviewer bias. The measurement of quality of life using the EORTC QLQ-C30 questionnaire results consists of two stages. The first stage involves calculating the raw score for each scale using Eq. 1. The second stage is the linear transformation stage, which involves standardizing the raw scores to obtain a score range of 1-100 using the linear transformation formula as seen in Eq. 2 and Eq. 3. Scores for all items range from 1 to 4, so the range is 3, except for items contributing to global health status (QoL), which are 7-point questions, so the range is 6 (18).
Eq. 1 | RS = raw score, P = value of each question, and n = total number of question; Eq. 2 l S = score for functional scale and RS = raw score; Eq. 3 l S = score for sympom and global health scale, and RS = raw score.
Quality of life categories were determined based on previous studies. For the functional scales, scores of ≤33 were classified as poor quality of life, 34-65 as moderate, and ≥66 as good quality of life. Conversely, for the symptom scales, scores of ≤33 indicated good quality of life, 34-65 indicated moderate, and ≥66 indicated poor quality of life.
Assessment of Adverse Drug Reactions, The FACT-ES questionnaire consists of 18 items that evaluate common endocrine-related symptoms associated with hormonal therapy, including vasomotor symptoms, musculoskeletal discomfort, fatigue, and gynecological complaints. Responses are rated on a five-point Likert scale, ranging from 0 (Not at all), 1 (A little), 2 (Somewhat), 3 (Quite a bit), to 4 (Very much). Higher scores indicate a greater severity of endocrine-related symptoms.
The total FACT-ES score was calculated by summing individual item scores, providing an overall measure of endocrine symptom burden. For analytical purposes, ADR severity was further categorized into mild, moderate, and severe levels based on the distribution of FACTES total scores and their impact on patients’ daily activities, in line with established principles of adverse drug reaction assessment. This categorization was informed by general principles of ADR severity assessment; however, it was not based on a formally validated or universally standardized cut-off system, which is acknowledged as a methodological limitation. The proportion of participants who reported no symptom at baseline (item rating = 0, “not at all”) then rated the symptom as present (≥1, “a little bit” or more severe) at month 3 was calculated for each item to identify newly emergent symptoms.
Given the use of interview-based data collection, the potential for recall bias cannot be excluded, particularly in the assessment of subjective symptoms and ADRs.
Handling of Missing Data
Missing data were assessed prior to analysis. Cases with incomplete key variables (e. g., missing clinical data or questionnaire responses) were excluded from the final analysis (complete case analysis). The proportion of missing data was minimal and therefore not subjected to imputation methods.
Data Analysis
Data analysis was performed using IBM SPSS Statistics software. Both descriptive and inferential statistical methods were applied. Descriptive statistics were used to summarize sociodemographic and clinical characteristics, treatment patterns, adverse drug reactions (ADRs), and quality of life (QoL) outcomes. Categorical variables were presented as frequencies and percentages, while continuous variables were expressed as mean values. Bivariate analysis was conducted to examine the associations between sociodemographic and clinical variables with type of therapy, survival duration, ADRs, and QoL. The Chi-square test or Fisher’s exact test was applied for categorical variables, as appropriate. The results were reported as odds ratios (ORs) with 95% confidence intervals (CIs), generated using SPSS. Multivariate analysis was performed using binary logistic regression in SPSS to identify independent predictors of QoL. QoL was dichotomized into poor-moderate and good categories. Variables with p-values < 0.25 in the bivariate analysis or those considered clinically relevant were included in the multivariate model. Adjusted odds ratios (AORs) with 95% confidence intervals were calculated to determine independent associations. A p-value of ≤ 0.05 was considered statistically significant.
Prior to the formal regression analysis, the fundamental assumptions of logistic regression were rigorously evaluated to ensure the integrity and reliability of the statistical inferences. Multicollinearity among the independent variables was systematically assessed using the variance inflation factor (VIF), and no significant multicollinearity was identified, as all values remained well within acceptable thresholds. The overall goodness of fit for the final model was further evaluated using the Hosmer-Lemeshow test to confirm that the predicted probabilities were consistent with the observed data. Additionally, the linearity of continuous variables with the logit of the outcome was assessed where applicable using the Box-Tidwell transformation. Adjusted odds ratios (AORs) accompanied by 95% confidence intervals were reported to quantify the strength of the associations, and a p-value ≤ 0.05 was strictly considered to be statistically significant. All statistical tests were two-tailed in nature and conducted using IBM SPSS Statistics software, ensuring a robust and standardized approach to the data analysis.
Results
Patient Sociodemographic and Clinical Characteristics
A total of 64 breast cancer patients receiving adjuvant endocrine therapy (AET) at Dr. Moewardi Regional General Hospital, Surakarta, were included in this study. The majority of patients were aged under 50 years, accounting for 60.9% of the total sample. In terms of disease stage, most patients were diagnosed at an advanced stage (III-IV), comprising 57.8% of cases, while the remaining patients were in the early stage (I-II).
The distribution of menopausal status showed a relatively balanced proportion between premenopausal and postmenopausal patients. Similarly, HER2 status was almost evenly distributed between negative and positive cases. Based on Table 1, statistical analysis indicated that there was no significant association between sociodemographic or clinical characteristics including age, cancer stage, menopausal status, HER2 status, and the type of therapy received (all p-values > 0.05).
| Variable | Hormonal Therapy N (%) | Chemo + Hormonal N (%) | OR (95% CI) | p-value |
|---|---|---|---|---|
| Sociodemographic Characteristics | ||||
| Age ≥ 50 years | 12 (54.5) | 10 (45.5) | 1.59 (0.72–3.51) | 0.253 |
| Age < 50 years | 16 (38.1) | 26 (61.9) | ||
| Cancer Stage | ||||
| Early stage (I-II) | 15 (55.6) | 12 (44.4) | 1.75 (0.79–3.88) | 0.165 |
| Advanced stage (III-IV) | 13 (35.1) | 24 (64.9) | ||
| Menopausal Status | ||||
| Premenopausal | 19 (45.2) | 23 (54.8) | 1.14 (0.49–2.66) | 0.757 |
| Postmenopausal | 9 (40.9) | 13 (59.1) | ||
| HER2 Status | ||||
| Negative | 14 (42.4) | 19 (57.6) | 0.86 (0.39–1.90) | 0.712 |
| Positive | 14 (45.2) | 17 (54.8) | ||
| Note: Association between sociodemographic and clinical characteristics with type of therapy (N = 64). OR, odds ratio; CI, confidence interval; HER2, human epidermal growth factor receptor 2. *p ≤ 0.05. | ||||
The survival analysis demonstrated that the vast majority of patients, comprising more than 90% of individuals across all investigated subgroups, had a treatment duration of less than five years, leaving only a small minority who survived beyond this specific threshold. Comprehensive statistical testing further revealed no significant associations between survival duration and any of the observed clinical or demographic variables, including patient age, cancer stage, menopausal status, and HER2 status (all p-values > 0.05). These findings, which highlight the lack of meaningful correlation between these parameters and long-term survival within the study population, are presented in detail within Table 2 for further academic review.
| Variable | < 5 years N (%) | > 5 years N (%) | OR (95% CI) | p-value |
|---|---|---|---|---|
| Sociodemographic Characteristics | ||||
| Age ≥ 50 years | 26 (89.7) | 3 (10.3) | 0.66 (0.17–2.60) | 0.547 |
| Age < 50 years | 32 (91.4) | 3 (8.6) | ||
| Cancer Stage | ||||
| Early stage (I-II) | 29 (90.6) | 3 (9.4) | 1.22 (0.31–4.85) | 0.774 |
| Advanced stage (III-IV) | 29 (90.6) | 3 (9.4) | ||
| Menopausal Status | ||||
| Premenopausal | 40 (90.9) | 4 (9.1) | 1.80 (0.45–7.21) | 0.401 |
| Postmenopausal | 18 (90.0) | 2 (10.0) | ||
| HER2 Status | ||||
| Negative | 30 (90.9) | 3 (9.1) | 1.40 (0.35–5.53) | 0.634 |
| Positive | 28 (90.3) | 3 (9.7) | ||
| Note: Association between sociodemographic and clinical characteristics with duration of therapy (<5 years vs >5 years) (N=64). OR, odds ratio; CI, confidence interval; HER2, human epidermal growth factor receptor 2. *p ≤ 0.05. | ||||
Treatment Patterns
Two main treatment approaches were identified in this study, namely combination chemotherapy and hormonal therapy, and hormonal therapy alone. Slightly more than half of the patients (51.6%) received combination therapy, while 48.4% received hormonal therapy alone.
Among patients undergoing chemotherapy, a variety of regimens were used. The most commonly administered regimen was cyclophosphamide combined with epirubicin (21.2%), followed by paclitaxel plus epirubicin and docetaxel plus epirubicin, each accounting for 18.1% of cases. Other regimens were used less frequently, including combinations involving carboplatin, trastuzumab, and cisplatin (Table 3).
| No. | Chemotherapy Regimen | Number (n) | Percentage (%) |
|---|---|---|---|
| 1 | Cyclophosphamide + Epirubicin | 7 | 21.2 |
| 2 | Paclitaxel + Epirubicin | 6 | 18.1 |
| 3 | Docetaxel + Epirubicin | 6 | 18.1 |
| 4 | Docetaxel + Carboplatin | 4 | 12.1 |
| 5 | Docetaxel | 2 | 6.1 |
| 6 | Docetaxel + Trastuzumab | 1 | 3.0 |
| 7 | Doxorubicin + Paclitaxel | 1 | 3.0 |
| 8 | Docetaxel + Trastuzumab + Cyclophosphamide | 1 | 3.0 |
| 9 | Paclitaxel + Cisplatin | 1 | 3.0 |
| 10 | Epirubicin + Cisplatin | 1 | 3.0 |
| 11 | Docetaxel + Cyclophosphamide | 1 | 3.0 |
| 12 | Epirubicin | 1 | 3.0 |
| 13 | Trastuzumab + Paclitaxel | 1 | 3.0 |
| Total Number | 33 | 100 | |
All patients in this study received tamoxifen as part of their hormonal therapy. The most frequently used regimen was tamoxifen combined with goserelin (42.2%), followed by tamoxifen monotherapy (26.6%). Additional combinations included tamoxifen with aromatase inhibitors such as anastrozole, letrozole, and exemestane, either alone or in combination with ovarian suppression (Table 4).
| No. | Hormonal Therapy Regimen | Number (n) | Percentage (%) |
|---|---|---|---|
| 1 | Tamoxifen + Zoladex (Goserelin) | 27 | 42.2 |
| 2 | Tamoxifen | 17 | 26.6 |
| 3 | Tamoxifen + Anastrozole + Zoladex | 7 | 10.9 |
| 4 | Tamoxifen + Anastrozole | 5 | 7.8 |
| 5 | Tamoxifen + Anastrozole (Arimidex) | 4 | 6.3 |
| 6 | Tamoxifen + Anastrozole + Exemestane (Aromasin) | 1 | 1.6 |
| 7 | Tamoxifen + Anastrozole + Arimidex | 1 | 1.6 |
| 8 | Tamoxifen + Capecitabine | 1 | 1.6 |
| 9 | Tamoxifen + Letrozole | 1 | 1.6 |
| Total Number | 64 | 100 | |
Adverse Drug Reactions
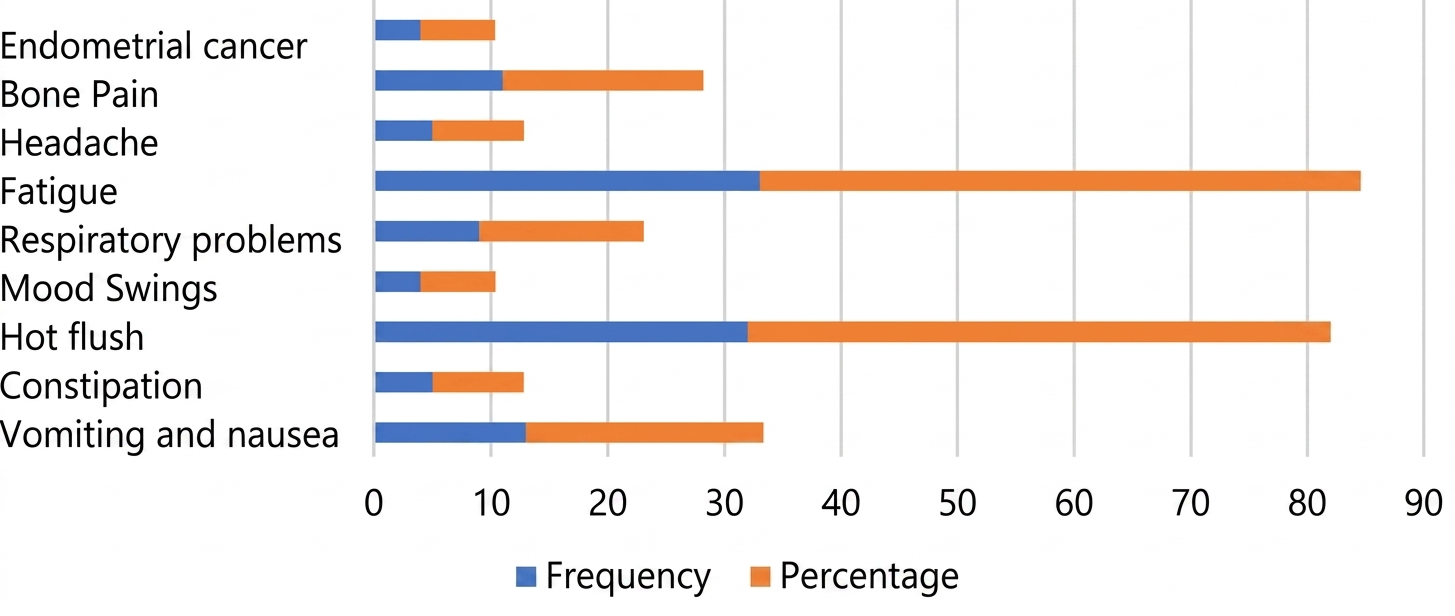
The profile of adverse drug reactions (Figure 2) showed that the most commonly reported symptoms were
fatigue (51.6%) and hot flushes (50%), particularly among patients receiving long-term hormonal therapy. Other
frequently reported complaints included nausea (20.3%) and bone or joint pain (17.2%). Less common but clinically
important adverse events included endometrial cancer, which was observed in 6.3% of patients during the treatment
period.
The analysis of factors associated with the severity of adverse drug reactions revealed that most patients experienced mild symptoms, while a smaller proportion reported severe symptoms requiring additional clinical attention. However, no statistically significant associations were identified between ADR severity and patient characteristics, including age, cancer stage, menopausal status, type of therapy, HER2 status, or survival duration (all p-values > 0.05), as shown in Table 5.
| Variable | ADRs Mild Symptoms (%) | ADRs Severe Symptoms (%) | OR (95% CI) | p-value |
|---|---|---|---|---|
| Age | ||||
| < 50 years | 29 (74.4) | 10 (25.6) | 1.31 (0.39-4.43) | 0.882 |
| ≥ 50 years | 19 (79.2) | 5 (20.8) | ||
| Cancer Stage | ||||
| Early stage (I-II) | 19 (70.4) | 8 (29.6) | 1.53 (0.49-4.80) | 0.465 |
| Advanced stage (III-IV) | 29 (78.4) | 8 (21.6) | ||
| Menopausal Status | ||||
| Premenopausal | 20 (71.4) | 8 (28.6) | 1.40 (0.45-4.35) | 0.553 |
| Postmenopausal | 28 (77.8) | 8 (22.2) | ||
| Type of Therapy | ||||
| Chemotherapy + hormonal therapy | 23 (75.8) | 8 (24.2) | 1.09 (0.35-3.39) | 0.885 |
| Hormonal therapy alone | 25 (74.2) | 8 (25.8) | ||
| HER2 Status | ||||
| Negative | 25 (75.8) | 8 (24.2) | 1.12 (0.36-3.48) | 0.842 |
| Positive | 23 (74.2) | 8 (25.8) | ||
| Survival Duration | ||||
| < 5 years | 43 (74.1) | 15 (25.9) | 1.18 (0.28-4.95) | 0.812 |
| ≥ 5 years | 5 (83.3) | 1 (16.7) | ||
| Note: Association between sociodemographic and clinical characteristics with adverse drug reactions (ADRs) severity (N=64). ADRs, adverse drug reactions; OR, odds ratio; CI, confidence interval; HER2, human epidermal growth factor receptor 2. *p ≤ 0.05. | ||||
Quality of Life
The assessment of quality of life using the EORTC QLQ-C30 instrument showed that the mean functional scale score was 79.65, indicating a generally good level of functioning. All functional domains, including physical, role, emotional, cognitive, and social functioning, demonstrated relatively high scores, suggesting that most patients were able to maintain daily activities and social roles despite ongoing treatment-related challenges.
The mean symptom scale score was 25.06, which was also categorized as good. However, certain symptoms were more prominent than others, particularly fatigue (38.02) and loss of appetite (38.54), both of which were categorized as moderate. Other symptoms, such as pain, nausea, sleep disturbances, constipation, diarrhea, and breathing difficulties, were generally mild.
| Scale | N | Mean | N (%) Score <33 | N (%) Score 34-65 | N (%) Score >66 |
|---|---|---|---|---|---|
| Functional Scale | |||||
| Physical Functioning | 64 | 75.73 (Good) | 0 (0) | 20 (30.8) | 44 (67.7) |
| Role Functioning | 64 | 74.48 (Good) | 1 (1.5) | 35 (53.8) | 28 (43.1) |
| Emotional Functioning | 64 | 77.73 (Good) | 0 (0) | 22 (33.8) | 42 (64.6) |
| Cognitive Functioning | 64 | 85.94 (Good) | 0 (0) | 17 (26.2) | 47 (72.3) |
| Social Functioning | 64 | 84.38 (Good) | 0 (0) | 21 (32.3) | 43 (66.2) |
| Average Score | 79.65 (Good) | ||||
| Symptom Scale | |||||
| Fatigue | 64 | 38.02 (Moderate) | 28 (43.1) | 36 (55.4) | 0 (0) |
| Pain | 64 | 16.67 (Good) | 61 (93.8) | 3 (4.6) | 0 (0) |
| Nausea | 64 | 27.60 (Good) | 53 (81.5) | 11 (16.9) | 0 (0) |
| Sleep Disturbance | 64 | 32.81 (Good) | 51 (78.5) | 10 (15.4) | 0 (0) |
| Loss of Appetite | 64 | 38.54 (Moderate) | 38 (58.5) | 26 (40.0) | 0 (0) |
| Constipation | 64 | 15.63 (Good) | 61 (93.8) | 3 (4.6) | 0 (0) |
| Diarrhea | 64 | 13.54 (Good) | 64 (98.5) | 0 (0) | 0 (0) |
| Breathing Problems | 64 | 16.15 (Good) | 57 (87.7) | 7 (10.8) | 0 (0) |
| Financial Problems | 64 | 26.56 (Good) | 49 (75.4) | 15 (23.1) | 0 (0) |
| Average Score | 25.06 (Good) | ||||
| Global Health Scale | |||||
| Global Health Status | 64 | 26.30 (Poor) | 49 (75.4) | 15 (23.1) | 0 (0) |
| Overall Health Score | 64 | 26.30 (Poor) | 50 (76.9) | 14 (21.5) | 0 (0) |
| Average Score | 26.30 (Poor) | ||||
| Quality of Life (QoL) | 64 | 76.38 (Moderate) | |||
| Note: Scores were based on EORTC QLQ-C30. Functional scales: higher scores = better functioning; symptom scales: higher scores = worse symptoms. Categories: ≤33 = poor, 34–65 = moderate, >66 = good. QoL, quality of life. | |||||
In contrast, the mean global health status score was 26.30, which falls into the poor category. Most patients (76.9%) reported a low overall perception of their health status, indicating a discrepancy between relatively good functional outcomes and poorer subjective health perception within the overall quality-of-life assessment framework.
Factors Associated with Quality of Life
Bivariate analysis demonstrated that cancer stage and type of therapy were significantly associated with quality of life. Patients with advanced-stage cancer were more likely to have poorer quality of life compared to those with early-stage disease (p = 0.010) across the evaluated functional and symptomatic domains.
Similarly, patients receiving combination chemotherapy and hormonal therapy had lower quality of life compared to those receiving hormonal therapy alone (p = 0.027) (Table 7) indicating a notable difference in patient-reported outcomes between treatment groups.
| Variable | Poor - Moderate (%) | Good (%) | OR (95% CI) | p-value |
|---|---|---|---|---|
| Age: <50 vs ≥50 years | 11 (44.0) / 29 (74.4) | 14 (56.0) / 10 (25.6) | 2.02 (0.86–4.75) | 0.071 |
| Stage: Early vs Advanced | 12 (44.4) / 28 (75.7) | 15 (55.6) / 9 (24.3) | 2.89 (1.25–6.67) | 0.010** |
| Menopause: Pre vs Post | 15 (53.6) / 25 (69.4) | 13 (46.4) / 11 (30.6) | 1.76 (0.78–3.98) | 0.089 |
| Therapy: Hormonal vs Combined | 14 (45.2) / 26 (78.8) | 17 (54.8) / 7 (21.2) | 2.74 (1.15–6.51) | 0.027* |
| HER2: Negative vs Positive | 17 (51.5) / 23 (74.2) | 16 (48.5) / 8 (25.8) | 1.68 (0.72–3.94) | 0.148 |
| Survival: < 5 vs ≥ 5 years | 38 (65.5) / 2 (33.3) | 20 (34.5) / 4 (66.7) | 0.74 (0.21–2.56) | 0.652 |
| Note: Association between sociodemographic/clinical characteristics and QoL (N = 64). OR: odds ratio; CI: confidence interval; HER2: human epidermal growth factor receptor 2. QoL: poor, moderate, good. *p ≤ 0.05, **p ≤ 0.01. | ||||
Multivariate logistic regression analysis confirmed that advanced-stage cancer and combination therapy remained significant predictors of poorer quality of life. Patients with advanced-stage disease had a significantly lower likelihood of achieving better quality of life (OR = 0.31; p = 0.004). Likewise, patients receiving combination therapy had reduced odds of better quality of life compared to those receiving hormonal therapy alone (OR = 0.44; p = 0.024). In contrast, age, menopausal status, HER2 status, and survival duration were not significantly associated with quality of life after adjustment for confounding variables (all pvalues > 0.05) (Table 8).
| Variable (Reference) | B | SE | Adjusted 95% CI (OR) | p-value |
|---|---|---|---|---|
| Age ≥50 years (vs <50) | -0.46 | 0.38 | 0.63 (0.30–1.32) | 0.155 |
| Advanced stage (III-IV) (vs early stage) | -1.18 | 0.42 | 0.31 (0.14–0.68) | 0.004** |
| Postmenopausal (vs premenopausal) | -0.44 | 0.34 | 0.64 (0.32–1.26) | 0.168 |
| Chemotherapy + hormonal (vs hormonal) | -0.82 | 0.39 | 0.44 (0.21–0.92) | 0.024* |
| HER2 positive (vs negative) | -0.48 | 0.36 | 0.62 (0.30–1.27) | 0.185 |
| Survival <5 years (vs ≥5 years) | -0.61 | 0.71 | 0.54 (0.13–2.21) | 0.384 |
| Note: Multivariate binary logistic regression analysis was performed to identify factors associated with quality of life (QoL). B, regression coefficient; SE, standard error; Adjusted OR, adjusted odds ratio; CI, confidence interval; HER2, human epidermal growth factor receptor 2. QoL was dichotomized into poor-moderate and good categories. Reference categories: age <50 years, early-stage cancer (I–II), premenopausal status, hormonal therapy alone, HER2 negative, and survival ≥5 years. *p ≤ 0.05, **p ≤ 0.01, ***p ≤ 0.001. *indicates statistically significant associations. | ||||
DISCUSSION
Sociodemographic and Clinical Characteristics
The findings of this study indicate that the majority of patients were aged < 50 years (60.9%) and were diagnosed at an advanced stage (57.8%). This pattern reflects the epidemiological characteristics of breast cancer in developing countries, where the age at diagnosis tends to be younger compared to developed countries. Recent global data from the World Health Organization and the International Agency for Research on Cancer indicate that breast cancer incidence in Asia is increasingly affecting women of productive age, with a lower median age compared to Western populations (1).
The high proportion of advanced-stage cases also suggests delays in diagnosis. Recent studies in Southeast Asia report that more than 50% of patients present at stages III– IV due to limited access to screening, low health literacy, and sociocultural barriers (19, 20). Such delays have a direct impact on prognosis and treatment options.
The absence of a significant association between sociodemographic characteristics and type of therapy suggests that treatment decisions are primarily driven by tumor biology rather than patient demographics. Current guidelines from the European Society for Medical Oncology and the National Comprehensive Cancer Network emphasize that adjuvant therapy selection is based on hormone receptor status, HER2 expression, and recurrence risk rather than age or menopausal status (21, 22).
Treatment Duration and Survival
Most patients had a treatment duration of less than five years, with no significant association observed with clinical variables. Clinically, endocrine therapy such as tamoxifen is recommended for at least 5-10 years to reduce recurrence and mortality (6, 23) in accordance with established international treatment guidelines.
However, long-term adherence remains a major challenge. Recent cohort studies report that approximately 30-50% of patients discontinue endocrine therapy before completing five years, primarily due to adverse effects and psychosocial factors (24, 25). This may explain why most patients in this study had not yet reached the optimal duration of therapy. The lack of association between clinical characteristics and survival duration is consistent with contemporary evidence suggesting that survival outcomes are influenced by complex interactions among treatment response, comorbidities, and healthcare access (26).
Treatment Patterns
The treatment patterns observed in this study indicate that combination chemotherapy and hormonal therapy were slightly more common than hormonal therapy alone. Chemotherapy regimens such as cyclophosphamide, epirubicin, and taxanes are wellestablished standards of care supported by robust clinical evidence (27, 28).
The use of targeted therapy such as trastuzumab in HER2-positive patients reflects current clinical practice. Recent studies have demonstrated that anti-HER2 therapies significantly improve disease-free survival and overall survival (29, 30).
All patients received tamoxifen as part of their endocrine therapy, which remains the standard treatment for premenopausal patients. The addition of ovarian suppression (e. g., goserelin) or aromatase inhibitors has been shown to provide additional benefits, particularly in high-risk patients (4, 31).
Adverse Drug Reactions (ADRs)
The most frequently reported adverse drug reactions were fatigue (51.6%) and hot flushes (50%). Hot flushes are a well-recognized side effect of endocrine therapy, particularly tamoxifen, due to estrogen modulation. Fatigue is also one of the most prevalent symptoms among cancer patients, affecting up to 60-80% of individuals undergoing treatment (32, 33).
Other symptoms, such as nausea and joint pain, were also observed, which are consistent with findings that chemotherapy and aromatase inhibitors may cause gastrointestinal disturbances and arthralgia (34, 35). The observed incidence of endometrial cancer (6.3%) in this study has important clinical implications; however, it must be interpreted with caution. In the existing literature, tamoxifen use has been associated with an increased risk of endometrial hyperplasia and carcinoma, particularly with prolonged exposure (36)(37). Nevertheless, the cross-sectional design of this study does not allow for the establishment of temporal or causal relationships between tamoxifen exposure and the occurrence of endometrial cancer (38). Furthermore, the relatively small sample size (N = 64) makes this proportion susceptible to random variation. The absence of a comparison group (e. g., patients not receiving tamoxifen or stratified by treatment duration) further limits the ability to estimate relative risk (39). Therefore, this finding should be interpreted as a descriptive observation indicating a potential clinical signal, rather than as a reliable estimate of prevalence or causal risk.
From a clinical perspective, this finding underscores the importance of routine gynecological monitoring in patients undergoing long-term endocrine therapy, particularly for the early detection of rare but serious adverse events.
Quality of Life (QoL)
One of the most notable findings in this study is the discrepancy between high functional scores (mean 79.65) and low global health status scores (mean 26.30). This finding requires a more critical interpretation based on the conceptual framework of the EORTC QLQ-C30 instrument. First, the functional scales primarily assess patients’ ability to perform daily activities (functional capacity), whereas the global health status reflects a broader, subjective perception of overall health and well-being (40, 41). These domains capture fundamentally different constructs and are not necessarily expected to align. Second, the low global health score observed in this study may reflect dimensions not directly measured, such as psychological distress, fear of cancer recurrence, or financial burden. However, since these variables were not explicitly assessed, such interpretations should be considered cautiously and not as definitive explanations. Third, although most symptom scores were categorized as mild, the presence of moderately severe symptoms particularly fatigue and appetite loss may disproportionately influence patients’ overall perception of health.
Previous studies have demonstrated that fatigue is one of the strongest determinants of reduced quality of life in cancer survivors, even when physical functioning remains relatively preserved (42).
Taken together, these findings highlight that subjective health perception is not solely determined by functional status, and that quality of life should be interpreted as a multidimensional construct encompassing both objective and subjective domains.
Factors Associated with Quality of Life
Bivariate analysis demonstrated that cancer stage and type of therapy were significantly associated with quality of life. Patients with advanced-stage cancer were more likely to experience poorer quality of life, which is consistent with studies showing that disease progression increases symptom burden and psychological distress (43). Patients receiving combination chemotherapy and hormonal therapy also had lower quality of life compared to those receiving hormonal therapy alone. This can be explained by the higher toxicity associated with chemotherapy, including neuropathy, nausea, and fatigue (44).
Multivariate analysis confirmed that advanced-stage disease (OR = 0.31; p = 0.004) and combination therapy (OR = 0.44; p = 0.024) were independent predictors of poorer quality of life. These findings are consistent with longitudinal studies demonstrating that treatment intensity is inversely associated with short-term quality of life (45, 46). In contrast, variables such as age, menopausal status, HER2 status, and survival duration were not significantly associated with quality of life after adjustment. This suggests that clinical factors play a more dominant role than demographic factors in determining quality of life among breast cancer patients (47).
The results indicate that advanced cancer stage and combination therapy are independent predictors of poorer quality of life. However, these associations should be interpreted in light of potential residual confounding. In clinical practice, combination chemotherapy and hormonal therapy are more commonly administered to patients with advanced disease or higher recurrence risk. Although multivariate analysis was conducted, not all relevant clinical variables (such as tumor burden, baseline performance status, or symptom severity at diagnosis) were available for adjustment. Therefore, the observed association between combination therapy and poorer quality of life may not be entirely independent of disease severity.
Additionally, the lack of statistically significant associations for variables such as age, menopausal status, HER2 status, and survival duration should be interpreted cautiously. Given the limited sample size, this study may be underpowered to detect modest associations (48).
Study Limitations
This study has several limitations. First, the cross-sectional design precludes the establishment of causal relationships between variables. Second, the relatively small sample size (N = 64) may limit statistical power and increase the risk of type II error. Third, the study was conducted at a single tertiary care center, which may limit the generalizability of the findings to other settings, particularly primary care or rural populations.
Additionally, important variables such as treatment adherence, psychological status, social support, and economic conditions were not comprehensively assessed, although these factors are known to significantly influence quality of life in cancer patients. Furthermore, the relatively short duration of follow-up and the predominance of patients with treatment duration <5 years limit the evaluation of long-term outcomes. Finally, the use of selfreported instruments may introduce subjective bias in the assessment of quality of life.
The relatively small sample size (N=64) represents a key limitation that may influence the robustness of the findings. Small sample sizes can lead to unstable estimates, wide confidence intervals, and reduced statistical power. In this context, interpretation of the results should not rely solely on statistical significance but also consider: the direction and magnitude of associations, and the consistency with existing evidence. To mitigate potential overfitting in logistic regression models, future studies may consider: limiting the number of variables included in the model, or applying alternative modeling strategies such as penalized regression techniques.
Conclusion
Combination chemotherapy and hormonal therapy showed a significant association with poorer quality of life compared to hormonal therapy alone (p = 0.027; OR = 2.74, 95% CI = 1.15-6.51). In addition, advanced-stage cancer was significantly associated with reduced quality of life (p = 0.010; OR = 2.89, 95% CI = 1.25-6.67). However, there were no significant associations between quality of life and age (p = 0.071), menopausal status (p = 0.089), HER2 status (p = 0.148), or survival duration (p = 0.652). Multivariate analysis confirmed that advanced-stage disease (p = 0.004; adjusted OR = 0.31, 95% CI = 0.14-0.68) and combination therapy (p = 0.024; adjusted OR = 0.44, 95% CI = 0.21-0.92) were independent predictors of poorer quality of life. In contrast, age (p = 0.155), menopausal status (p = 0.168), HER2 status (p = 0.185), and survival duration (p = 0.384) were not significantly associated after adjustment. Although the overall functional scale indicated good patient functioning (mean = 79.65), the global health status score remained low (mean = 26.30), highlighting a discrepancy between objective functional outcomes and subjective health perception. Fatigue (mean = 38.02) and loss of appetite (mean = 38.54) were the most prominent symptoms affecting patients’ well-being.
Advanced stage disease and combination chemotherapy hormonal therapy were identified as independent predictors of poorer quality of life among breast cancer patients. Although functional scores were generally high, the persistently low global health status indicates a gap between maintained daily functioning and patients’ overall health perception, likely driven by symptom burden such as fatigue and appetite loss. These findings suggest that treatment intensity and disease progression have a measurable impact on patientreported outcomes, beyond sociodemographic factors.
Clinically, these results support the need for routine integration of patient-reported outcome measures and symptom management, particularly in patients receiving combination therapy. However, given the cross-sectional design, single-center setting, and limited sample size, the findings should be interpreted cautiously. External validity may be limited, and broader applicability requires confirmation in larger, multicenter, and longitudinal studies.
Declarations
Acknowledgment
We would like to express our sincere gratitude to the Directorate General of Higher Education, Research, and Technology, Ministry of Education, Culture, Research, and Technology, for providing financial support for this research. This study was funded under Decree Number 0419/C3/DT.05.00/2025 and the following research grant agreements/contracts: 127/C3/DT.05.00/PL/2025; 043/LL6/PL/AL.04/2025; and 046/UDB.LPPM/A.34-HK/V/2025.
Conflict of Interest
The authors declare no conflicting interest.
Data Availability
All data generated or analyzed during this study are included in this published article.
Ethics Statement
This study received ethical approval from the Health Research Ethics Committee of Dr. Moewardi Hospital, Surakarta, under approval number 1.287/VI/HREC/2025. All participants were provided with a clear explanation of the study objectives, procedures, potential risks, and benefits prior to enrollment. Written informed consent was obtained from all participants before data collection.
Funding Information
This work was supported by the Directorate General of Higher Education, Research, and Technology, Ministry of Education, Culture, Research, and Technology under Grant Number 0419/C3/DT.05.00/2025 and the following research grant agreements/contracts: 127/C3/DT.05.00/PL/2025; 043/LL6/PL/AL.04/2025; and 046/UDB.LPPM/A.34-HK/V/2025.
References
- Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, et al. Cancer statistics for the year 2020: An overview. Intl Journal of Cancer. 2021;149(4):778-789. doi: https://doi.org/10.1002/ijc.33588
- DeSantis CE, Ma J, Gaudet MM, Newman LA, Miller KD, Goding Sauer A, et al. Breast cancer statistics, 2019. CA A Cancer J Clinicians. 2019;69(6):438-451. doi: https://doi.org/10.3322/caac.21583
- Indonesia PK. PROFIL KESEHATAN INDONESIA 2023. 2023.
- Francis PA, Pagani O, Fleming GF, Walley BA, Colleoni M, Láng I, et al. Tailoring Adjuvant Endocrine Therapy for Premenopausal Breast Cancer. N Engl J Med. 2018;379(2):122-137. doi: https://doi.org/10.1056/nejmoa1803164
- Harbeck N, Penault-Llorca F, Cortes J, Gnant M, Houssami N, Poortmans P, et al. Breast cancer. Nat Rev Dis Primers. 2019;5(1):66. doi: https://doi.org/10.1038/s41572-019-0111-2
- Pan H, Gray R, Braybrooke J, Davies C, Taylor C, McGale P, et al. 20-Year Risks of Breast-Cancer Recurrence after Stopping Endocrine Therapy at 5 Years. N Engl J Med. 2017;377(19):1836-1846. doi: https://doi.org/10.1056/nejmoa1701830
- Henry NL, Unger JM, Schott AF, Fehrenbacher L, Flynn PJ, Prow DM, et al. Randomized, Multicenter, Placebo-Controlled Clinical Trial of Duloxetine Versus Placebo for Aromatase Inhibitor–Associated Arthralgias in Early-Stage Breast Cancer: SWOG S1202. Jco. 2018;36(4):326-332. doi: https://doi.org/10.1200/jco.2017.74.6651
- Zwart W, Terra H, Linn SC, Schagen SB. Cognitive effects of endocrine therapy for breast cancer: keep calm and carry on?. Nat Rev Clin Oncol. 2015;12(10):597-606. doi: https://doi.org/10.1038/nrclinonc.2015.124
- Haggstrom LR, Vardy JL, Carson EK, Segara D, Lim E, Kiely BE. Effects of Endocrine Therapy on Cognitive Function in Patients with Breast Cancer: A Comprehensive Review. Cancers. 2022;14(4):920. doi: https://doi.org/10.3390/cancers14040920
- Cheng KKF, Wong WH, Koh C. Unmet needs mediate the relationship between symptoms and quality of life in breast cancer survivors. Support Care Cancer. 2015;24(5):2025-2033. doi: https://doi.org/10.1007/s00520-015-2994-0
- Ng CG, Mohamed S, Kaur K, Sulaiman AH, Zainal NZ, Taib NA. Perceived distress and its association with depression and anxiety in breast cancer patients. PLoS ONE. 2017;12(3):e0172975. doi: https://doi.org/10.1371/journal.pone.0172975
- Ursem CJ, Bosworth HB, Shelby RA, Hwang W, Anderson RT, Kimmick GG. Adherence to Adjuvant Endocrine Therapy for Breast Cancer: Importance in Women with Low Income. Journal of Women's Health. 2015;24(5):403-408. doi: https://doi.org/10.1089/jwh.2014.4982
- Nekhlyudov L, Mollica MA, Jacobsen PB, Mayer DK, Shulman LN, Geiger AM. Developing a Quality of Cancer Survivorship Care Framework: Implications for Clinical Care, Research, and Policy. JNCI: Journal of the National Cancer Institute. 2019;111(11):1120-1130. doi: https://doi.org/10.1093/jnci/djz089
- Basch E, Deal AM, Kris MG, Scher HI, Hudis CA, Sabbatini P, et al. Symptom Monitoring With Patient-Reported Outcomes During Routine Cancer Treatment: A Randomized Controlled Trial. Jco. 2016;34(6):557-565. doi: https://doi.org/10.1200/jco.2015.63.0830
- Rowland JH, Bellizzi KM. Cancer Survivorship Issues: Life After Treatment and Implications for an Aging Population. Jco. 2014;32(24):2662-2668. doi: https://doi.org/10.1200/jco.2014.55.8361
- Alfano CM, Jefford M, Maher J, Birken SA, Mayer DK. Building Personalized Cancer Follow-up Care Pathways in the United States: Lessons Learned From Implementation in England, Northern Ireland, and Australia. American Society of Clinical Oncology Educational Book. 2019.(39):625-639. doi: https://doi.org/10.1200/edbk_238267
- Permata A, Perwitasari DA, Candradewi SF, Septiantoro BP, Purba FD. Penilaian Kualitas Hidup Pasien Kanker Nasofaring Dengan Menggunakan EORTC QLQ-C30 di RSUP dr. Kariadi Semarang. J. Pharm. Sci. Clin. Res. 2022;7(1):39. doi: https://doi.org/10.20961/jpscr.v7i1.43764
- Fallowfield LJ, Leaity SK, Howell A, Benson S, Cella D. Assessment of quality of life in women undergoing hormonal therapy for breast cancer: validation of an endocrine symptom subscale for the FACT‐B. Breast Cancer Res Treat. 1999;55(2):187-197. doi: https://doi.org/10.1023/a:1006263818115
- Lim YX, Lim ZL, Ho PJ, Li J. Breast Cancer in Asia: Incidence, Mortality, Early Detection, Mammography Programs, and Risk-Based Screening Initiatives. Cancers. 2022;14(17):4218. doi: https://doi.org/10.3390/cancers14174218
- Fan L, Strasser-Weippl K, Li JJ, St Louis J, Finkelstein DM, Yu KD, et al. Breast cancer in China. The Lancet Oncology. 2014;15(7):e279-e289. doi: https://doi.org/10.1016/s1470-2045(13)70567-9
- Cardoso F, Kyriakides S, Ohno S, Penault-Llorca F, Poortmans P, Rubio I, et al. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology. 2019;30(8):1194-1220. doi: https://doi.org/10.1093/annonc/mdz173
- Gradishar WJ, Moran MS, Abraham J, Abramson V, Aft R, Agnese D, et al. Breast Cancer, Version 3.2024, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network. 2024;22(5):331-357. doi: https://doi.org/10.6004/jnccn.2024.0035
- Harvey B, DeMichele A, Henry L, Burstein H. Endocrine and Targeted Therapy for HR-Positive, HER2-Negative Metastatic Breast Cancer – Capivasertib-Fulvestrant: Rapid Guideline Update. ASCO Podcast DO Group. 2024; 42(12):1450-1453. doi: https://doi.org/10.1200/gdl.24.03132
- Thorén L, Margolin S, Eliasson E, Bergh J, Lindh JD. Adherence to endocrine therapy in early breast cancer in relation to Cytochrome P450 2D6 genotype: a comparison between pharmacy dispensation data and medical records. Breast Cancer Res Treat. 2023;198(3):499-508. doi: https://doi.org/10.1007/s10549-023-06887-2
- Collin LJ, Cronin-Fenton DP, Ahern TP, Goodman M, McCullough LE, Waller LA, et al. Early Discontinuation of Endocrine Therapy and Recurrence of Breast Cancer among Premenopausal Women. Clinical Cancer Research. 2021;27(5):1421-1428. doi: https://doi.org/10.1158/1078-0432.ccr-20-3974
- Waks AG, Winer EP. Breast Cancer Treatment. Jama. 2019;321(3):288. doi: https://doi.org/10.1001/jama.2018.19323
- Gradishar WJ, Moran MS, Abraham J, Abramson V, Aft R, Agnese D, et al. NCCN Guidelines® Insights: Breast Cancer, Version 4.2023. Journal of the National Comprehensive Cancer Network. 2023;21(6):594-608. doi: https://doi.org/10.6004/jnccn.2023.0031
- Bhimani J, O’Connell K, Persaud S, Blinder V, Burganowski RP, Ergas IJ, et al. The landscape of use of NCCN-guideline chemotherapy regimens in stage I-IIIA breast cancer in an integrated healthcare delivery system. Breast Cancer Res Treat. 2024;208(2):405-414. doi: https://doi.org/10.1007/s10549-024-07433-4
- Swain SM, Baselga J, Kim SB, Ro J, Semiglazov V, Campone M, et al. Pertuzumab, Trastuzumab, and Docetaxel in HER2-Positive Metastatic Breast Cancer. N Engl J Med. 2015;372(8):724-734. doi: https://doi.org/10.1056/nejmoa1413513
- Modi S, Jacot W, Yamashita T, Sohn J, Vidal M, Tokunaga E, et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med. 2022;387(1):9-20. doi: https://doi.org/10.1056/nejmoa2203690
- Burstein HJ, Lacchetti C, Griggs JJ. Adjuvant Endocrine Therapy for Women With Hormone Receptor–Positive Breast Cancer: ASCO Clinical Practice Guideline Focused Update. Jop. 2019;15(2):106-107. doi: https://doi.org/10.1200/jop.18.00617
- Bower JE. Cancer-related fatigue—mechanisms, risk factors, and treatments. Nat Rev Clin Oncol. 2014;11(10):597-609. doi: https://doi.org/10.1038/nrclinonc.2014.127
- Mustian KM, Alfano CM, Heckler C, Kleckner AS, Kleckner IR, Leach CR, et al. Comparison of Pharmaceutical, Psychological, and Exercise Treatments for Cancer-Related Fatigue. JAMA Oncol. 2017;3(7):961. doi: https://doi.org/10.1001/jamaoncol.2016.6914
- Kim S, Chen N, Reid P. Current and future advances in practice: aromatase inhibitor–induced arthralgia. Rheumatology Advances in Practice. 2024;8(2): rkae024. doi: https://doi.org/10.1093/rap/rkae024
- Yu K, Portes P, Morris GS, Huang L, Felix ER, Farkas GJ, et al. The role of exercise in aromatase inhibitor‐induced arthralgia. PM&R. 2024;16(12):1406-1416. doi: https://doi.org/10.1002/pmrj.13193
- Felix AS, Cook LS, Gaudet MM, Rohan TE, Schouten LJ, Setiawan VW, et al. Abstract A114: The etiology of uterine sarcomas: A pooled analysis of the epidemiology of endometrial cancer consortium (E2C2). Cancer Prevention Research. 2012;5(11_Supplement):A114-A114. doi: https://doi.org/10.1158/1940-6207.prev-12-a114
- Emons G, Mustea A, Tempfer C. Tamoxifen and Endometrial Cancer: A Janus-Headed Drug. Cancers. 2020;12(9):2535. doi: https://doi.org/10.3390/cancers12092535
- Zhong J, Cai B, Su T, Chen H. The association between metabolic syndrome and incidence of endometrial cancer: a meta-analysis. Diabetol Metab Syndr. 2025;17(1):430. doi: https://doi.org/10.1186/s13098-025-01964-6
- Grimes DA, Schulz KF. Bias and causal associations in observational research. The Lancet. 2002;359(9302):248-252. doi: https://doi.org/10.1016/s0140-6736(02)07451-2
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ. Quality of Life Questionnaire-Cancer 30. PsycTESTS Dataset. 1993. doi: https://doi.org/10.1037/t01822-000
- Collins G, Bottomley A, Fayers P, de Graeff A, Groenvold M, Petersen M, et al. Pcn17: psychometric properties of the eortc quality of life core questionnaire (qlq-c30) in eortc trials. Value in Health. 2001;4(6):437-438. doi: https://doi.org/10.1016/s1098-3015(11)71577-7
- Lipscomb J, Gotay CC, Snyder CF. Patient-reported Outcomes in Cancer: A Review of Recent Research and Policy Initiatives. CA: A Cancer Journal for Clinicians. 2007;57(5):278-300. doi: https://doi.org/10.3322/ca.57.5.278
- Sharma N, Purkayastha A. Factors affecting quality of life in breast cancer patients: A descriptive and cross-sectional study with review of literature. J Mid-life Health. 2017;8(2):75. doi: https://doi.org/10.4103/jmh.jmh_15_17
- Lavoie Smith EM, Barton DL, Qin R, Steen PD, Aaronson NK, Loprinzi CL. Assessing patient-reported peripheral neuropathy: the reliability and validity of the European Organization for Research and Treatment of Cancer QLQ-CIPN20 Questionnaire. Qual Life Res. 2013;22(10):2787-2799. doi: https://doi.org/10.1007/s11136-013-0379-8
- Park K, Loibl S, Sohn J, Park Y, Jiang Z, Tadjoedin H, et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the diagnosis, treatment and follow-up of patients with early breast cancer. ESMO Open. 2024;9(5):102974. doi: https://doi.org/10.1016/j.esmoop.2024.102974
- D’Arienzo A, Verrazzo A, Pagliuca M, Napolitano F, Parola S, Viggiani M, et al. Toxicity profile of antibody-drug conjugates in breast cancer: practical considerations. eClinicalMedicine. 2023;62:102113. doi: https://doi.org/10.1016/j.eclinm.2023.102113
- Svensson M, Strand GC, Bonander C, Johansson N, Jakobsson N. Analyses of quality of life in cancer drug trials - a review of measurements and analytical choices in post-reimbursement studies. BMC Cancer. 2024;24(1):311. doi: https://doi.org/10.1186/s12885-024-12045-8
- Carnahan RM, Brown GD. The power and pitfalls of underpowered studies. Pharmacotherapy. 2024;44(9):698-700. doi: https://doi.org/10.1002/phar.4605