RESEARCH ARTICLE
Evaluation of Antibiotic Use in Pediatric Patients with Bronchopneumonia Hospitalized at K. R. M. T Wongsonegoro Hospital
Academic Editor: Pilli Govindaiah
Sciences of Pharmacy|Vol. 5, Issue 3, pp. 303-311 (2026)
CC BY 4.0-2026 Authors
Views
Downloads
Shares
Received
Feb 22, 2026Revised
Mar 17, 2026Accepted
Jun 21, 2026Published
Jul 14, 2026
Abstract
Bronchopneumonia is a respiratory tract infection affecting the bronchi and lungs and remains one of the leading causes of mortality among children worldwide. Antibiotics are the mainstay of therapy; however, their high utilization necessitates evaluation to ensure rational use. At K. R. M. T. Wongsonegoro Hospital, Semarang, bronchopneumonia was the leading infectious disease among pediatric patients in 2023, highlighting the need for a comprehensive assessment of antibiotic prescribing practices. This study aimed to determine the profile of antibiotic use and evaluate both qualitative and quantitative appropriateness of antibiotic therapy among pediatric inpatients with bronchopneumonia. A descriptive, retrospective, cross-sectional study was conducted involving 281 pediatric inpatients aged 0–18 years hospitalized with bronchopneumonia throughout 2023. Qualitative antibiotic appropriateness was evaluated using the Gyssens method, while quantitative utilization was analyzed via the Defined Daily Dose (DDD)/100 inpatient-days system. Ceftriaxone was the predominant therapy, both as monotherapy and in combination with azithromycin. Qualitative analysis revealed notable irrationalities, characterized primarily by incorrect dosing intervals and inappropriate dosages, alongside truncated treatment durations. Quantitatively, ceftriaxone exhibited the highest consumption rate, dominating the Drug Utilization 90% (DU90%) segment. These findings reveal suboptimal antibiotic utilization patterns, underscoring an urgent need for institutional prescription audits and targeted educational interventions to mitigate the risk of localized antimicrobial resistance.
Introduction
Bronchopneumonia is a term used to describe inflammation that occurs in the walls of the bronchioles and surrounding lung tissue. Bronchopneumonia is also known as lobular pneumonia, because inflammation occurs in the lung parenchyma that is permanent in the bronchioles and surrounding alveoli (1). Bronchopneumonia is caused by bacterial, viral, or fungal infections in the bronchioles and surrounding lung tissue (2).
Pneumonia is the leading cause of death among children compared to other infectious diseases, with more than 700,000 children under the age of five dying each year—or about 2,000 deaths per day. Of these, approximately 190,000 occur among newborns. Most of these deaths are actually preventable. Globally, the incidence of pneumonia exceeds 1,400 cases per 100,000 children, equivalent to 1 case for every 71 children per year. The highest incidence rates are found in South Asia, at approximately 2,500 cases per 100,000 children, followed by West and Central Africa with approximately 1,620 cases per 100,000 children (3). Pneumonia can occur in all age groups, but the highest number of deaths occur in infants and children, because the body's immune response system is weakened and not yet fully developed (4). According to a report by the Indonesian Ministry of Health in 2020, bronchopneumonia is including diseases commonly found in infants and children, with a very high number of cases, reaching 808,694 deaths in children under the age of 5 (5).
In 2020, pneumonia was among the top 10 causes of hospital admission across various regions in Indonesia. Pneumonia also accounts for a high mortality rate worldwide, ranking as the 8th leading cause of death in the United States and is associated with high healthcare costs. These high costs are also linked to the prolonged use of antibiotics even when patients have low risk and few comorbidities, so the rational use of antibiotics in pneumonia requires further attention (6).
In 2022, the national coverage of pneumonia in toddlers was 38.8%. Central Java Province still ranks 9th with the highest number of pneumonia cases in Indonesia, with a prevalence of 43.5% of the population. Based on data from the Semarang City Health Office in 2022, pneumonia continues to experience a 5% increase in the number of infant and child deaths from 2017 to 2022 (7). Based on the results of a pre-survey on bronchopneumonia at the K.R.M.T Wongsonegoro General Hospital in Semarang City, it was found that this disease is most commonly found in children. It ranks first as a pediatric infectious disease.
Bronchopneumonia is treated with antibiotics. The high use of antibiotics has led to various conflicts, posing a risk that affects health issues related to bacterial resistance to antibiotics. The cause of antibiotic resistance is the inappropriate use of antibiotics. Antibiotic resistance can lead to treatment failure, resulting in unsuccessful patient recovery and increased mortality (8). Based on previous research (9) on the Evaluation of Rationality in Clinical Outcomes of Antibiotic Use and Patterns of Bacterial Resistance to Antibiotics in Children with Pneumonia, the antibiotics with the highest resistance are ampicillin at 65%, ampicillin sulbactam at 66.67%, and ceftriaxone at 40.74%.
Evaluation of antibiotic use is one of the measures to prevent bacterial resistance to antibiotics. The rationality of antibiotic administration can be evaluated qualitatively and quantitatively. Quantitative evaluation uses the ATC/DDD method, while qualitative evaluation is based on predetermined drug criteria. Thus, to determine the quality of antibiotic use, an evaluation is carried out using the Gyssens method (10). Health workers have a big responsibility in preventing antibiotic resistance, so it's important to improve people's knowledge and awareness about the proper use of antibiotics (11). The results of a systematic review of 48 articles evaluating antibiotic use in hospitalized pneumonia patients indicate that the quantitative analysis of the results shows that ceftriaxone and meropenem antibiotics were the top choices, with values of 1547.735 DDD/100 bed days and 3011.2 DDD/1000 patient days, respectively. Evaluation of the quality of antibiotic use showed the highest level irrational in category (IVa) at 67.6% (12).
The study was conducted to determine the qualitative and quantitative evaluation results of antibiotic use in pediatric patients with bronchopneumonia admitted to K.R.M.T Wongsonegoro Regional General Hospital in 2023. While broad epidemiological data emphasizes the global and national burden of pediatric pneumonia, local management strategies often suffer from a paucity of empirical data regarding actual prescribing behavior in clinical practice. Prior studies frequently separate quantitative consumption from qualitative clinical appropriateness. By simultaneously deploying the ATC/DDD method and the Gyssens framework in a primary regional hospital, this study addresses an essential research gap, providing the granular insights required to design actionable, setting-specific antibiotic stewardship interventions where clinical susceptibility data is limited
Methodology
Study Design and Location
The study was conducted using a descriptive research design with a cross-sectional approach. Data collection was performed retrospectively. The data collected were medical records of pediatric patients with bronchopneumonia from January to December 2023 at K.M.R.T Wongsoneoro Regional General Hospital.
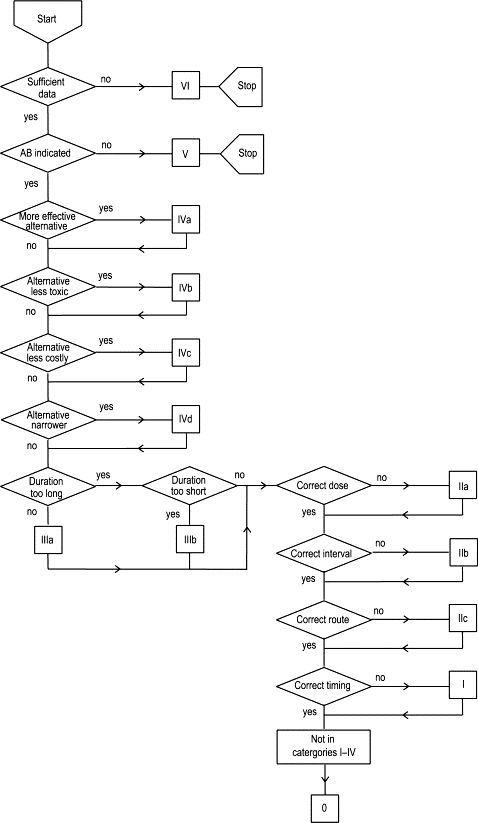
The tools used in this study were data collection sheets designed according to the researchers' needs to conduct qualitative antibiotic evaluation using the Gyssens method and quantitative evaluation using the ATC/DDD and DU90 methods. In addition, the Gyssens flowchart (Figure 1) was used for qualitative evaluation, while the 2023 Guideline for ATC classification and DDD assignment and the WHO website https://atcddd.fhi.no/atc_ddd_index/ were used for quantitative evaluation. Ministry of Health Regulation No. 28 of 2021 on Guidelines for Antibiotic Use was also used as a guide in evaluating antibiotic use in patients with bronchopneumonia by examining the type of antibiotic, dose, interval, route, duration, and safety of the antibiotics administered to patients (13). The material used in the study was the medical records of pediatric bronchopneumonia patients who were hospitalized at K.R.M.T Wongsonegoro Hospital from January to December 2023.
Population & Sample
The study population initially comprised 948 patients, from which a final sample size of 281 patients was selected based on specific eligibility criteria. The inclusion criteria required subjects to be pediatric inpatients aged 0–18 years diagnosed with bronchopneumonia who received antibiotic therapy between January and December 2023, underwent empirical or definitive antibiotic treatment for a maximum duration of 14 days, and possessed complete and clear medical records. Conversely, patients were excluded from the study if they discontinued treatment voluntarily, died during their hospital stay, were referred to other healthcare facilities, or presented with concurrent infectious diseases.
The study was conducted with a preparatory stage that included an observational study on the use of antibiotics in pediatric patients with bronchopneumonia, which showed a significant number. Next, data on antibiotic use was collected from medical records. The data was then analyzed univariately, namely with descriptive analysis to determine the pattern of antibiotic use and patient characteristics, which were presented in Table 1 and Table 2. Qualitative analysis used the Gyssens flowchart and was then grouped according to category. The Gyssens qualitative assessment was conducted independently by trained clinical pharmacists utilizing a standardized data extraction form to minimize subjectivity. To ensure internal consistency, a random sample of 10% of the medical records underwent a secondary, independent cross-check by a senior clinical pharmacist; any discrepancies in category assignment were resolved by consensus. While a formal, multi-center external validation process was outside the scope of this retrospective review, this rigorous internal audit protocol preserved data accuracy. Quantitative analysis used ATC/DDD. This study has been approved by the Medical/Health Research Bioethics Commission of the Faculty of Medicine, UNISSULA, with No. 469/XI/2024/KomisiBioetik.
Results and Discussion
The study was conducted on 281 medical records of pediatric bronchopneumonia patients who were hospitalized at K.M.R.T Wongsonegoro General Hospital from January to December 2023 and met the inclusion and exclusion criteria of the study. The demographic characteristics of the patients, consisting of gender and age, are presented in Table 1. The results showed that there were more male patients (152 patients, 54.09%) than female patients. Male patients have a higher risk of developing bronchopneumonia because their respiratory tract is narrower than that of female patients. In addition, they also play outdoors more often than female patients (15).
| Characteristic | Number of patients | Percentages |
|---|---|---|
| Gender | ||
| Male | 152 | 54.09% |
| Female | 129 | 45.91% |
| Total | 281 | 100% |
| Age | ||
| Newborn (0–28 days) | 2 | 0.71% |
| Infant (>28 days – 12 months) | 108 | 38.08% |
| Toddler (>12 – 23 months) | 0 | 0.00% |
| Preschool child (2–5 years) | 118 | 41.99% |
| School age child (6–11 years) | 45 | 16.01% |
| Adolescents (12–18 years) | 9 | 3.20% |
| Total | 281 | 100% |
Patients aged 2 - 5 years accounted for the highest number compared to other age groups. This age group is more susceptible to bronchopneumonia because they have lower immunity compared to those aged over 5 years (17). This is supported by data from the 2023 Central Java Provincial Health Profile, which shows that cases of pneumonia among children under 5 increased by approximately 3.63% compared to the previous year, totaling 134,708 cases. In fact, pneumonia is the leading cause of death among children under 5 in Central Java Province, accounting for 26.76% of all deaths(18). At this age, a person's immune system is not yet optimal and the humoral immune response in increasing antibody levels is still limited. The relatively narrow respiratory tract is also one of the causes of a higher risk of children being susceptible to infectious diseases, especially those transmitted through the air (19).
Based on the study, data was obtained on the use of antibiotics in patients, both those given singly and in combination which were presented in Table 2. The most widely used single antibiotic was ceftriaxone, which was used in 187 patients (61.11%), while the most widely used combination was ceftriaxone + azithromycin in 25 patients (8.17%). Previous research conducted in the inpatient ward of Ciamis Regional General Hospital showed that single-dose ceftriaxone was prescribed in 88.03% of cases. This antibiotic has a broad spectrum of both gram-positive and gram-negative bacteria (20). Ceftriaxone is also used as an empirical antibiotic for infants and children who are hospitalized and have not received complete immunizations, so it can be used as a treatment option for pediatric patients who cannot receive penicillin (21).
| Type | Antibiotic | Total | Persentages |
|---|---|---|---|
| Single | Ceftriaxone | 187 | 61.11% |
| Cefotaxime | 39 | 12.75% | |
| Azithromycin | 10 | 3.27% | |
| Amoxicillin | 2 | 0.65% | |
| Combination | Ceftriaxone + Azithromycin | 25 | 8.17% |
| Cefotaxime + Gentamicin | 15 | 4.90% | |
| Ceftriaxone + Gentamicin | 15 | 4.90% | |
| Cefotaxime + Azithromycin | 8 | 2.61% | |
| Ceftriaxone + Amoxicilin | 2 | 0.65% | |
| Ceftriaxone + Cefotaxime | 1 | 0.33% | |
| Cefotaxime + Gentamicin + Azithromycin | 1 | 0.33% | |
| Ceftriaxone + Meropenem + Amikacin | 1 | 0.33% | |
| Total | 306 | 100% | |
Combination therapy is also given to some patients, with the aim of enhancing the effectiveness of antibiotics in specific infections (synergistic effect) and slowing down and minimizing the occurrence of infection. Combination therapy can be used as empirical therapy in severe infections or when it is possible that the infection is caused by more than one bacterium. The selection of combination therapy can be based on the way antibiotics work on different targets, which can enhance or interfere with the overall activity of antibiotics. Combination therapy is most commonly used in pediatric bronchopneumonia at K.R.M.T Wongsonegoro General Hospital, namely ceftriaxone + azithromycin with a percentage of 10.32%. In line with research in eastern Ethiopia, the combination of ceftriaxone + azithromycin is most commonly used in the treatment of pneumonia, with a percentage of 46.5% (22). Ceftriaxone shows broader activity against gram-negative bacteria compared to generations I and II, and the addition of azithromycin (macrolide class) improves coverage of atypical pathogens compared to β-lactam monotherapy. The combination of ceftriaxone and azithromycin works in two different ways, producing a synergistic effect for the treatment of pneumonia. Ceftriaxone works by inhibiting cell wall synthesis, while azithromycin inhibits bacterial protein synthesis. In addition, azithromycin has an immunomodulatory effect, which can reduce the inflammatory effects of antibacterial activity (23). The use of a combination of beta-lactam antibiotics and macrolides is one of the options for empirical treatment regimens in pediatric pneumonia when monotherapy is insufficiently effective(24).
Quantitative Antibiotic Evaluation
Quantitative evaluation of antibiotic use can be performed using the ATC/DDD method in accordance with WHO recommendations. The purpose of this evaluation is to measure the amount of antibiotics used at the prescribed daily dose (DDD/100 patient days) based on criteria established by the WHO (14). The antibiotics used in the research sample included 8 antibiotics and were classified under the ATC code, consisting of ceftriaxone, cefotaxime, azithromycin, gentamicin, amoxicillin, meropenem, and amikacin. The ATC code in the table was used to classify antibiotics based on the DDD value in grams (g).
The results showed that the total DDD value in pediatric patients with bronchopneumonia at K.R.M.T Wongsonegoro Hospital from January to December 2023 was 51.48 DDD/100 patient days (Table 3). Ceftriaxone was the most frequently administered antibiotic, accounting for 815.15 g, whereas amoxicillin oral had lowest usage, at 3.6 g. From a clinical perspective, interpreting a DDD value of 40.83 within a pediatric population requires careful nuance. Since the WHO assigns a standard adult dose of 2 grams as the benchmark DDD for ceftriaxone, and pediatric doses are weight-dependent and significantly lower, this elevated metric underscores an intense, concentrated exposure to broad-spectrum agents within the ward. This pattern suggests an institutional over-reliance on third-generation cephalosporins for empirical treatment. While national guidelines recommend narrow-spectrum beta-lactams like amoxicillin as first-line empiric choices for uncomplicated pneumonia, the widespread selection of ceftriaxone appears to be driven by dosing convenience (once-daily administration) and an empirical strategy to cover potential resistance. However, this practice creates an escalating loop of selective pressure, contributing directly to the 40.74% ceftriaxone resistance rates reported in regional literature, and highlights a critical target for antimicrobial stewardship programs to enforce de-escalation protocols.
| No | ATC Code | Antibiotic Name | Route | DDD WHO standard (gram) (WHO, 2023) | Amount of antibiotic use (gram) | Total LOS (days) | DDD/100 Hospitalization days |
|---|---|---|---|---|---|---|---|
| 1. | J01DD04 | Ceftriaxone | P | 2 | 815.15 | 998 | 40.83 |
| 2. | J01DD01 | Cefotaxime | 4 | 138.165 | 3.46 | ||
| 3. | J01FA10 | Azithromycin | 0.5 | 11.625 | 2.32 | ||
| 4. | J01GB03 | Gentamicin | 0.24 | 3.985 | 1.66 | ||
| 5. | J01CA04 | Amoxicillin | 3 | 5.25 | 0.17 | ||
| 6. | J01DH02 | Meropenem | 3 | 1.5 | 0.05 | ||
| 7. | J01GB06 | Amikacin | 1 | 0.8 | 0.08 | ||
| 8. | J01FA10 | Azithromycin | O | 0.3 | 8.01 | 2.67 | |
| 9. | J01CA04 | Amoxicillin | 1.5 | 3.6 | 0.24 | ||
| Total | 51.48 | ||||||
| Note: P = parenteral and O = oral. | |||||||
The results also show that the antibiotics used and included in the 90% segment are ceftriaxone (PO), ceftriaxone (PO), azithromycin (IV), and gentamicin (PO). Meanwhile, the antibiotics used in the 10% segment are amoxicillin and azithromycin (PO). Antibiotics included in the 90% DU segment are the most frequently prescribed antibiotics, while antibiotics included in the 10% DU segment are rarely prescribed (25). In a study conducted by Ceftriaxone consistently entered the 90% DU profile during the 2013–2017 period. Its broad spectrum makes this antibiotic useful as empirical therapy in various cases of infection (26).
Several factors can affect antibiotic utilization, including hospital policies on antibiotic use, patient clinical conditions, and the prescribing physician’s preferences. Rational antibiotic prescribing is generally reflected by lower levels of use, while elevated Defined Daily Dose (DDD) values may suggest irrational prescribing practices (27). Based on the 2021 WHO AWaRe (Access, Watch, Reserve) classification, ceftriaxone and azithromycin are categorized as “Watch” antibiotics, meaning that these antibiotics have a high potential to cause antimicrobial resistance. Therefore, their use requires monitoring to prevent excessive use (28).
| No | Antibiotic name | Route | DDD/100 Patient-days | DU 90% (%) | Segment |
|---|---|---|---|---|---|
| 1 | Ceftriaxone | P | 40.83 | 79.31 | 90% |
| 2 | Cefotaxime | P | 3.46 | 6.72 | |
| 3 | Azithromycin | O | 2.67 | 5.19 | |
| 4 | Azithromycin | P | 2.32 | 4.51 | |
| 5 | Gentamicin | P | 1.66 | 3.22 | |
| 6 | Amoxicillin | O | 0.24 | 0.47 | 10% |
| 7 | Amoxicillin | P | 0.33 | 0.16* | |
| 8 | Amikacin | P | 0.08 | - | |
| 9 | Meropenem | P | 0.10 | - | |
| Total | 51.48 | 100% | |||
| Note: P = parenteral and O = oral. | |||||
Qualitative Antibiotic Evaluation
Qualitative evaluation was conducted using the Gyssens method. Based on the results of the study, there were several irrational uses in patients, as shown in Table 5. The duration of antibiotic administration is categorized as too short if it is given for a period shorter than the existing treatment guidelines. The results of the study show that there were 25 (8.9%) antibiotics received by patients with a shorter duration, thus falling into category III b. The largest group consisted of patients who received ceftriaxone for only 1 day (9 patients) and 2 days (1 patient), followed by those who received gentamicin for only 1 day (4 patients) and 2 days (2 patients), azithromycin for only 1 day (5 patients), and cefotaxime for 1 day (4 patients). Antibiotics were received by patients in < 3 days, and this duration did not comply with the guidelines, because clinical monitoring, laboratory tests, and other supporting examinations are evaluated at least every 3 days (13). The use of antibiotics for a shorter duration than that specified in the treatment guidelines can increase the risk of side effects and bacterial resistance. This is in line with research (29) that inappropriate administration of antibiotics can increase unwanted side effects and make microorganisms resistant to antibiotics.
Antibiotic dosage inaccuracy occurs when the amount administered does not fall within the recommended dosage range, either in the form of an overdose or an underdose. Administering antibiotics in doses that exceed the recommended range can cause toxicity, while administering antibiotics in doses lower than the minimum level risks causing treatment failure (30). When administering antibiotics to children, dose adjustments must take into account body weight and age. In the results of the evaluation of Table 5, it was found that 51 (18.15%) patients received antibiotic with an inappropriate dose thus falling into category II a. Dosing inaccuracies include overdoses and underdoses. Inappropriate antibiotic dosing can potentially reduce the success of therapy and trigger antibiotic resistance. In addition, the body's immune system can be weakened by inappropriate use, and several side effects can arise from inappropriate antibiotic administration (31).
| Category | Gyssens criteria | Number | Percentages |
|---|---|---|---|
| 0 | Rational | 131 | 46.62% |
| III b | Treatment duration too short | 25 | 8.90% |
| II a | Inappropriate dosage | 51 | 18.15% |
| II b | Inappropriate dosing interval | 74 | 26.33% |
| Total | 281 | 100% | |
Antibiotic use is categorized as inappropriate interval if the time between antibiotic doses does not comply with the recommended interval in the therapy guidelines, whether given at too short or too long intervals (Anggraini, 2021). The results of the evaluation in Table 5 of the studies included in category IIb were 74 (26.33%). Incorrect dosing intervals occurred in patients receiving ceftriaxone; according to antibiotic guidelines, the recommended dosing interval is every 12 hours, but 57 patients received the antibiotic every 24 hours and 1 patient received it every 8 hours. Another antibiotic administered at an incorrect interval was cefotaxime, which should have been administered every 8 hours; however, 15 patients received the antibiotic every 12 hours. Incorrect dosing intervals also occurred in 1 patient who received gentamicin every 12 hours, whereas the recommended interval is every 24 hours.The use of antibiotics at inappropriate intervals, when administration times are inconsistent, can result in irregular increases in blood drug levels. This condition prevents the achievement of the steady state level required for antibiotics to work optimally in killing microorganisms(10).
Limitations
A limitation of this study includes its retrospective, single-center design, which may restrict the immediate generalizability of the findings to other healthcare facilities. Furthermore, while rigorous internal duplicate reviews were executed by clinical pharmacists to assign Gyssens classifications, a formal external multi-rater validation process was not performed. Future prospective multicenter initiatives should integrate external validation frameworks to further strengthen antibiotic audit tools.
Conclusion
In conclusion, this study demonstrates a profound institutional reliance on ceftriaxone for pediatric bronchopneumonia, evidenced by its highest consumption rate of 40.83 DDD/100 patient-days and its dominance within the Drug Utilization 90% (DU90%) segment along with cefotaxime and oral azithromycin. Qualitative evaluation via the Gyssens method exposed critical gaps in rational prescribing, driven largely by inappropriate dosing intervals (26.33%) and incorrect dosages (18.15%). These findings indicate that antibiotic deployment remains suboptimal and poses a distinct risk for accelerating localized antimicrobial resistance. To safeguard therapeutic efficacy, the hospital must immediately transition from descriptive monitoring to active antimicrobial stewardship. This should include enforcing strict, weight-based pediatric electronic prescribing alerts, implementing mandatory 72-hour clinical de-escalation audits, and providing ongoing clinician education aligned with national therapeutic guidelines
Abbreviations
ATC = Anatomical Therapeutic Chemical; DDD/100 = Defined Daily Dose per 100; DU 90% = Drug Utilization 90%; WHO = World Health Organization; LOS = Length of Stay; P = Parenteral; O = Oral.
Declarations
Acknowledgment
The author would like to express his gratitude to the Director of K.R.M.T Wongsonegoro Hospital for granting research permission and assisting in the collection of research samples.
Conflict of Interest
The authors declare no conflicting interest.
Data Availability
The data generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
This observational study was approved by the Medical/Health Research Bioethics Commission of the Faculty of Medicine, UNISSULA, with No. 469/XI/2024/KomisiBioetik.
Funding Information
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
References
- Fathurrahman MH, Simanjuntak N, Sopiah NS. Analisis efektivitas biaya penggunaan obat pada pasien rawat inap penyakit covid-19 kategori suspek non-comorbid dengan terapi obat kombinasi antivirus dan antibiotik di salah satu rumah sakit kota bandung periode juli – desember 2021. Pharma Xplore. 2023;8(1):24-34. doi: https://doi.org/10.36805/jpx.v8i1.5251
- Cristanti FF, Mahmudiono T, Erfiana. Proses Asuhan Gizi Terstandar pada Pasien Pediatri Bronkopneumonia dan Kejang Demam Sederhana Pasca Konvulsi dengan Pemberian Diet Tinggi Kalori dan Tinggi Protein: Sebuah Laporan Kasus. Mgk. 2024;13(1):276-285. doi: https://doi.org/10.20473/mgk.v13i1.2024.276-285
- 3. World Health Organization. Pneumonia in Children. Geneva: World Health Organization; 2022 (cited 2026, January 18). Available from: https://www.who.int/news-room/fact-sheets/detail/pneumonia
- Hatim F. Kemenkes RI. 2022. hal. 1 World Pneumonia Day 2022. Tersedia pada: https://yankes.kemkes.go.id/view_artikel/1997/world-pneumonia-day-2022
- Alvionita V, Sulfatimah S, Astuti A, Nurfitri N. Hubungan Status Gizi Dan Status Imunisasi Dengan Kejadian Pneumonia Pada Bayi. Ahmar Metastasis Health J. 2022;1(4):137-143. doi: https://doi.org/10.53770/amhj.v1i4.92
- Pedoman Dokter Paru Indonesia. Pedoman Diagnosis dan Penatalaksanaan Pneumonia Komunitas di Indonesia. Jakarta: Perhimpunan Dokter Paru Indonesia; 2022.
- Halida F, Sudiro S, Sugiarto J. Evaluasi Kebijakan Perencanaan Obat Instalasi Farmasi Dinas Kesehatan Kota Semarang. Jurnal Manajemen Kesehatan Indonesia. 2017;5(1):6-11. doi: https://doi.org/10.14710/jmki.5.1.2017.6-11
- Faradita N, Yulia R, Herawati F. Profil penggunaan antibiotik pada pasien pneumonia di komunitas: tinjauan pustaka. Intisari Sains Medis. 2022;13(2):340-345. doi: https://doi.org/10.15562/ism.v13i2.1312
- Elvionita C, Sari IP, Nuryastuti T. Evaluation the Rationality of Clinical Outcomes of Antibiotic Use and Patterns of Bacterial Resistance to Antibiotics in Children with Pneumonia. Majalah Farmaseutik. 2023;19(1):131-139. doi: https://doi.org/10.22146/farmaseutik.v19i1.76103
- Anggraini W, Candra TM, Maimunah S, Sugihantoro H. Evaluasi Kualitatif Penggunaan Antibiotik pada Pasien Infeksi Saluran Kemih dengan Metode Gyssens. kesdok. 2020;2(1):1-8. doi: https://doi.org/10.24123/kesdok.v2i1.2876
- Arfianto E, Hadi Sulistyaningrum I, Pribadi P, Lutfiyati H, Eka Septiana V, Ratna Puspitadewi A, et al. A Survey of Community Perceptions and Knowledge Toward Antibiotic Resistance: Case Study in Magelang, Indonesia. BIO Web Conf. 2023;75:05002. doi: https://doi.org/10.1051/bioconf/20237505002
- Syam RA, Karuniawati H. Antibiotic Evaluation Of Hospitalized Pneumonia Patients Using Gyssen or DDD 100 Bed Days or DDD 1000 Patient Days : Review. Pharmacon J Farm Indones. 2024;21(1):49–64.
- Kemenkes RI. Peraturan Menteri Kesehatan Republik Indonesia Nomor 28 Tahun 2021 Tentang Pedoman Penggunaan Antibiotik. Jak; 2021: pp 1–98.
- Novekawati. Implementasi peraturan menteri kesehatan republik indonesia nomor 24 tahun 2022 tentang rekam medis. legalita. 2023;5(1):64-72. doi: https://doi.org/10.47637/legalita.v5i1.869
- Firdaus FS, Chundrayetti E, Nurhajjah S. Hubungan Status Gizi, Umur, dan Jenis Kelamin dengan Derajat Pneumonia pada Balita di RSUP Dr. M. Djamil Padang Periode Januari 2018 – Desember 2018. Jikesi. 2021;2(1):143-150. doi: https://doi.org/10.25077/jikesi.v2i1.418
- Batchelor HK, Marriott JF. Paediatric pharmacokinetics: key considerations. Brit J Clinical Pharma. 2015;79(3):395-404. doi: https://doi.org/10.1111/bcp.12267
- Gangga Dewi MKP, Anak Agung Oka Lely, Anak Agung Ayu Lila Paramasatiari. Karakteristik Penderita Pneumonia Usia 1-59 Bulan yang Dirawat Inap di Rumah Sakit. amj. 2023;3(3):316-322. doi: https://doi.org/10.22225/amj.3.3.2023.316-322
- Prastiwi SAT, Handayani HR. Pengaruh Belanja Pemerintah Bidang Pendidikan, Kesehatan dan PDRB Terhadap IPM di Provinsi Jawa Tengah (Studi Kasus 35 Kab/kota Provinsi Jawa Tengah). Dipo. J. Econ. 2024;10(3):135-147. doi: https://doi.org/10.14710/djoe.39681
- Rachmawati S, Masito DK, Rachmawati E. Evaluasi Penggunaan Antibiotik Pada Pasien Anak Rawat Inap di RSD Dr. Soebandi Jember. Jfg. 2020;6(2):212-220. doi: https://doi.org/10.22487/j24428744.v.i.14976
- Poen A. Evaluasi penggunaan antibiotik pada pasien pneumonia di ruang instalasi rawat inap rumah sakit x. Scpij. 2023;7(1):15-22. doi: https://doi.org/10.52447/scpij.v7i1.6014
- Indriyani D, Hartianty EP. Profil Penggunaan Antibiotika Pada Pasien Anak Balita Penderita Bronkopneumonia Di Instalasi Rawat Inap Rumah Sakit X Daerah Indramayu. jff. 2023;1(1):14-32. doi: https://doi.org/10.35760/jff.2023.v1i1.8048
- Jambo A, Edessa D, Adem F, Gashaw T. Appropriateness of antimicrobial selection for treatment of pneumonia in selected public hospitals of Eastern Ethiopia: A cross-sectional study. SAGE Open Medicine. 2023;11:1-11. doi: https://doi.org/10.1177/20503121231163792
- Hikmah N, Andayani TM, Puspitasari I. Comparison of effectiveness and safety between ceftriaxone/azithromycin and levofloxacin in hospitalized CAP patients: a review. Majalah Farmaseutik. 2024;20(3):382. doi: https://doi.org/10.22146/farmaseutik.v20i3.94147
- Schwinghammer TL, DiPiro JT, Ellingrod V, DiPiro CV. DiPiro's Pharmacotherapy Handbook. 12th ed. New York: McGraw Hill; 2023.
- Zahra NL, Yuniarti E, Ainni AN, Fitri D. Evaluasi penggunaan antibiotik pada pasien pneumonia dengan metode atc/ddd dan du 90% di rawat inap rumah sakit umum purbowangi periode tahun 2020-2022. UJP. 2023:2(4):535-542. doi: https://doi.org/10.23917/ujp.v2i4.169
- Saepudin S, Sendysagita C, Yuniarti E. Drug Utilization 90% Profile of Antibiotics Use during the Period of 2013 – 2017 at a Private Teaching Hospital in Yogyakarta. J.Pharm.Sci.Community. 2022;19(1):8-14. doi: https://doi.org/10.24071/jpsc.003061
- Suri N, Junando M, Afriyana R. A Comprehensive Evaluation of Antibiotic Usage: Establishing a Foundation for Effective Antimicrobial Stewardship. Jfiki. 2024;11(3):298-311. doi: https://doi.org/10.20473/jfiki.v11i32024.298-311
- Zanichelli V, Sharland M, Cappello B, Moja L, Getahun H, Pessoa-Silva C, et al. The <i>WHO AWaRe (Access, Watch, Reserve) antibiotic book</i> and prevention of antimicrobial resistance. Bull World Health Org. 2023;101(04):290-296. doi: https://doi.org/10.2471/blt.22.288614
- Herawati D, Azzahra DN, Farhah HD, Hadi JCH, Sagala JT, Rosadi NC, et al. Efek samping penggunaan antibiotik irasional pada gangguan pernapasan infeksi saluran penafasan akut. jikep. 2023;9(2):464-471. doi: https://doi.org/10.33023/jikep.v9i2.1500
- Febby Valentine Purwadi RKS. Penggunaan Obat Off-label pada Anak-Anak. Farmaka [Internet]. 2018;16(Vol 16, No 1 (2018): Farmaka (Juni)):54–60. Tersedia pada: http://jurnal.unpad.ac.id/farmaka/article/view/16843
- Adelia D, Nofrika V, Thama AE. Gambaran penggunaan antibiotik oral tanpa resep dokter pada masyarakat rw 010 kelurahan jatinegara kecamatan cakung. J Farm IKIFA. 2021;1(1):53–63. Available from: https://epik.ikifa.ac.id/jfi/article/view/31