REVIEW
Medicinal Plants with Psychoactive Properties: A Comprehensive Review
Academic Editor: Bharath Kumar Chagaleti
Sciences of Phytochemistry|Vol. 5, Issue 2, pp. 262-282 (2026)
CC BY 4.0-2026 Authors
Views
Downloads
Shares
Received
Feb 24, 2026Revised
Apr 24, 2026Accepted
Jun 10, 2026Published
Jul 12, 2026
Abstract
Medicinal plants have been used in traditional medicine to alleviate a range of neurological and psychological disorders. Numerous plant-derived phytochemicals are known to modulate central nervous system activity by interacting with neurotransmitters, receptors, and neurochemical pathways. This review provides a comprehensive overview of medicinal plants with psychoactive properties, their major bioactive constituents, mechanisms of action, therapeutic potential, toxicity concerns, and regulatory considerations. Literature was collected from scientific databases, including PubMed, Scopus, ScienceDirect, Web of Science, and Google Scholar, using relevant keywords on psychoactive medicinal plants and neuropharmacological activities. Twenty medicinal plants commonly associated with anxiolytic, antidepressant, sedative, hallucinogenic, or cognition-enhancing effects were reviewed. Major phytochemical classes identified included alkaloids, flavonoids, terpenoids, phenolic compounds, cannabinoids, and saponins. Several plants, such as Withania somnifera, Cannabis sativa, Valeriana officinalis, Psilocybe cubensis, and Passiflora incarnata, have been reported to exhibit neuropharmacological activities in preclinical and limited clinical studies, through modulation of serotonergic, dopaminergic, GABAergic, and endocannabinoid systems. In addition to psychoactive effects, many reviewed plants exhibited antioxidant, anti-inflammatory, neuroprotective, and adaptogenic properties. However, despite promising pharmacological findings, most available evidence remains preclinical, with limited clinical validation regarding efficacy, safety, standardization, and long-term use. This review highlights the therapeutic prospects and current limitations of psychoactive medicinal plants and emphasizes the need for further experimental and clinical investigations for safe and evidence-based therapeutic applications.
Keywords:
Introduction
Mental health represents a fundamental aspect of overall human well-being and significantly influences emotional stability, cognition, behavior, decision-making, and the ability to cope with daily stress. Being an integral part of our health, mental health condition significantly affects one’s quality of life. It helps us to understand our potential, to work efficiently and to ensure social contributions (1, 2). Mental disorders are generally characterized by abnormalities in emotional regulation, cognitive processes, or behavior that interfere with normal psychological functioning and daily activities (3). Among the most frequently reported psychiatric conditions are depression, anxiety disorders, schizophrenia, bipolar disorder, obsessive-compulsive disorder (OCD), and post-traumatic stress disorder (PTSD) (4). Recent reports from the National Institutes of Health (NIH) indicate that mental illnesses affect a substantial proportion of the adult population in the United States, emphasizing the increasing global burden of neuropsychiatric disorders (5). Psychoactive medications are substances capable of modifying mood, perception, consciousness, cognition, and behavior through their effects on the central nervous system (6, 7). Conventional psychoactive medications, including antidepressants, anxiolytics, antipsychotics, and mood stabilizers, are widely prescribed for the treatment of psychiatric illnesses (8). Despite their therapeutic importance, many synthetic psychoactive drugs are associated with undesirable effects such as dizziness, sedation, agitation, cognitive impairment, metabolic disturbances, and dependency-related complications (9). Moreover, inconsistent therapeutic responses and concerns regarding long-term safety continue to limit their clinical utility in some patients.
Medicinal plants have long been incorporated into traditional healthcare practices for the management of neurological and psychological disorders. Several plant species used in traditional systems such as Ayurveda have been reported to possess calming, cognition-enhancing, anxiolytic, antidepressant, and neuroprotective properties. For example, medicinal plants such as Brahmi and Ashwagandha have been reported to exhibit scientific attention because of their potential neuropharmacological effects (10). Various plant parts, including leaves, roots, bark, seeds, and fruits, contain bioactive phytochemicals such as alkaloids, flavonoids, phenolic compounds, terpenoids, saponins, and volatile oils that may influence brain function and neurotransmitter activity (11, 12). Several plant-derived psychoactive compounds have been reported to exert multiple neuropharmacological effects, including anxiolytic, antidepressant, sedative, stimulant, hallucinogenic, and cognition-enhancing activities. These effects are believed to occur through interactions with neurotransmitter systems and signaling pathways involving serotonin, dopamine, gamma-aminobutyric acid (GABA), glutamate, and acetylcholine (13, 14).
Although some medicinal plants have demonstrated relatively favorable tolerability in experimental and limited clinical investigations, their pharmacological efficacy and safety may vary depending on dosage, phytochemical composition, duration of use, and individual biological response. In addition, important concerns related to toxicity, pharmacokinetics, standardization, abuse potential, and regulatory control remain inadequately explored for many psychoactive medicinal plants. Although previous review articles have discussed certain medicinal plants or isolated psychoactive constituents, a comprehensive and balanced overview integrating therapeutic potential, mechanisms of action, safety considerations, toxicity profiles, and regulatory perspectives remains limited. Therefore, the present review aims to critically summarize medicinal plants reported to possess psychoactive properties, with emphasis on their major phytochemical constituents, neuropharmacological activities, therapeutic significance, safety concerns, and future research prospects in the field of neuropharmacology and mental health research.
Methodology
This study was designed as a comprehensive narrative review rather than a formal systematic review or meta-analysis. To enhance methodological transparency, selected principles of the PRISMA 2020 guidelines were considered during the literature search, screening, and study selection process. Relevant scientific publications were collected from October 2024 to July 2025 using electronic databases, including PubMed, Scopus, ScienceDirect, and Web of Science. Google Scholar was also explored as an additional source to identify relevant publications that might not have been indexed in the major databases.
The literature search strategies were developed using combinations of keywords and Boolean operators related to psychoactive medicinal plants and neuropharmacological activities. The main search query included terms such as (“medicinal plant” OR “herbal plant” OR phytomedicine) AND (“psychoactive” OR “psychotropic” OR hallucinogenic OR anxiolytic OR antidepressant) AND (“phytochemicals” OR “bioactive compounds” OR “traditional medicine”). Additional keywords including “sedative,” “neuroprotective,” “cognitive enhancement,” and “central nervous system” were incorporated when necessary to broaden the search coverage.
Research articles published from 2015 to 2025 were primarily prioritized to ensure inclusion of recent scientific evidence, while a few earlier studies were retained to provide historical and conceptual background. Only peer-reviewed English-language publications describing psychoactive, anxiolytic, antidepressant, sedative, hallucinogenic, or cognition-enhancing properties of medicinal plants or their active phytochemicals were considered suitable for inclusion. Studies were excluded if they were duplicates, non-English articles, conference abstracts, editorials, dissertations, unreliable online materials, or studies relying exclusively on molecular docking without pharmacological or experimental support. Screening was initially performed through assessment of titles and abstracts, followed by full-text assessment of potentially relevant articles. The final selection of literature was assessed by the authors to ensure scientific relevance and consistency with the objectives of the review.
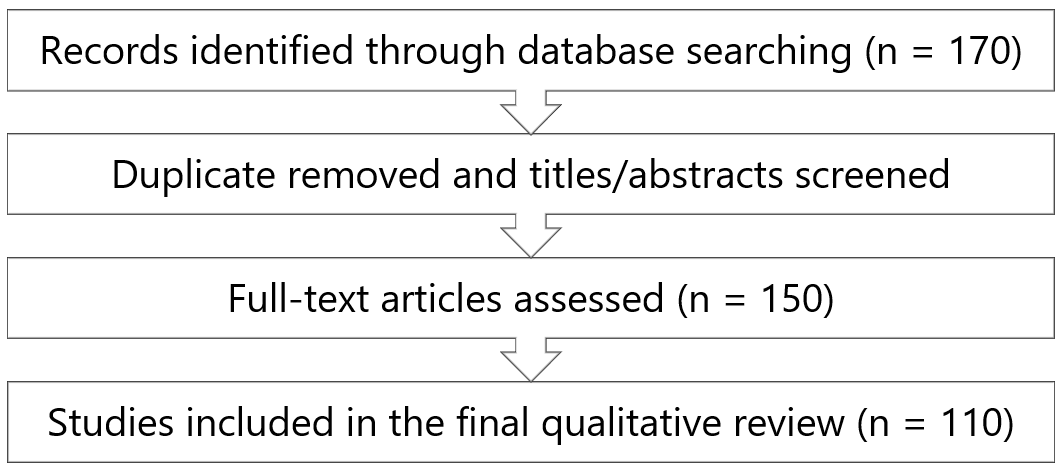
The literature screening procedure was carried out in two stages. Initially, the titles and abstracts of the retrieved studies were examined to assess their relevance to the scope of the review. Articles were then selected based on their scientific relevance, methodological reliability, and alignment with the objectives of the study. The preliminary database search identified approximately 170 records. After removal of duplicate entries and initial screening, 150 articles remained eligible for full-text evaluation, of which 110 studies were ultimately included in the final qualitative review.
The collected information was analyzed through a qualitative approach and organized based on plant origin, major phytochemical compounds, mechanisms underlying psychoactive activity, therapeutic potential, toxicity profiles, and regulatory aspects. Due to considerable differences in study design, experimental procedures, and reported outcomes across the selected literature, conducting a quantitative meta-analysis was not considered feasible. A formal risk-of-bias assessment was not conducted because the included literature comprised diverse types of evidence, including narrative reviews, ethnopharmacological reports, in vitro studies, animal-based experiments, and limited clinical studies, which were not appropriate for standard bias assessment methods. A simplified overview of the literature identification and screening procedure used in this comprehensive review is presented in Figure 1.
Medicinal Plants with Psychoactive Properties
The three main categories of naturally occurring psychoactive substances are hallucinogens, cannabinoids, and opioids (15). Hallucinogens have the potential to cause the most profound psychological changes like changes in mood, awareness, and perception, which can lead to synesthesia, vivid visual hallucinations, and a distorted perspective of space and time (16). Psilocybe genus "magic mushrooms", nutmeg and ergot are well-known natural sources of hallucinogens (17). On the other hand, cannabinoids are a complex group of molecules that comprise phytocannabinoids, endocannabinoids, and synthetic cannabinoids. Cannabinoids are phytochemicals that act on cannabinoid receptors (CB1 and CB2) and play an important role in the central nervous system (CNS) and immune system. The main psychoactive compounds are Δ9-tetrahydrocannabinol (Δ9-THC) and cannabidiol (CBD), which may produce opposite effects on human brain function. Cannabinoids are derived from the Cannabis sativa (marijuana) have shown therapeutic potential in the management of disorders such as schizophrenia, Parkinson’s disease, Alzheimer’s disease, epilepsy, depression, and anxiety disorders (15, 18, 19). Finally, opioids are those compounds derived from the poppy plant (Papaver somniferum) as well as semisynthetic and synthetic substances with comparable characteristics that have the ability to interact with opioid receptors in the brain. Drugs like morphine, codeine, and fentanyl are frequently used to treat pain because of the analgesic and sedative properties of opioids (20).
From the above discussion, we can summarize psychoactive substances into three categories found in various plants, their possible psychoactive effects as summarized in Table 1.
| Type of psychoactive compounds | Source | Major Chemical constituents | Psychoactive Effects | References |
|---|---|---|---|---|
| Hallucinogen | Ayahuasca, Psilocybe genus, Ergot Etc. | N, N-dimethyltryptamine, psilocybin, dimethyl tryptamine | Synesthesia, Vivid Visual Hallucinations, Distorted Time Perception, Altered awareness | (21) |
| Cannabinoid | Cannabis sativa (marijuana) | Δ9-tetrahydrocannabinol (Δ9-THC) and cannabidiol (CBD), phytocannabinoids, endocannabinoids | Antidepressant. Anxiolytic. Used in schizophrenia, Parkinson’s disease, Alzheimer’s disease, Epilepsy. | (15, 18, 19) |
| Opioid | Papaver somniferum (poppy plant) | Morphine, codeine, and fentanyl | Sedation | (20) |
Common Medicinal Plants with Psychoactive Properties in nature:
In this review twenty (20) renowned medicinal plants are studied which possess phytochemicals with psychoactive activities. Most of them are often used in our cuisine as spices or as medicine for different therapeutic purposes.
Myristica fragrans: Myristica fragrans (Houtt. ) is known to as nutmeg locally and belongs to Myristicaceae family (Figure 2). It is an evergreen tree indigenous to the Maluku Islands in Indonesia, and has been widely used in Indian traditional medicine to cure a variety of diseases (22).
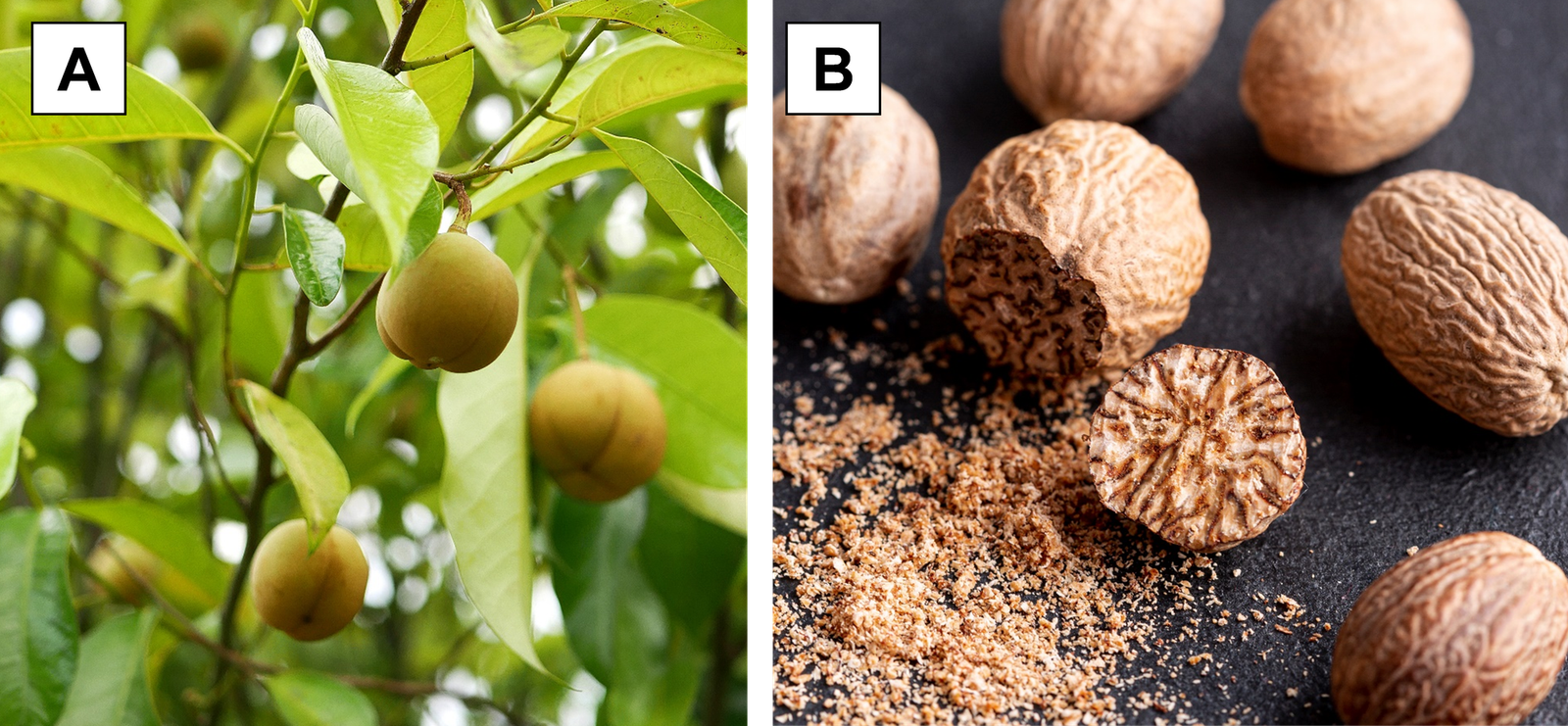
Nutmeg seeds have shown psychoactive action and are known for their sedative, hallucinogenic, antidepressant and anxiolytic properties. Approximately 5-7 g of ground nutmeg seeds may produce these psychogenic effects (23). Nutmeg seed contains 20-40% of essential oil, with myristicin (11.17%), myristic acid (39.93%), and elemicin (22.16%) identified as the major constituents (24). Nutmeg seed extract may stimulate serotonin release and promote relaxation and drowsiness through interaction with the brain’s endocannabinoid system. Therefore, it may have potential benefits in managing insomnia, anxiety, and behavioral agitation (25). Besides their psychogenic effects, nutmeg seeds have also shown antioxidant, anti-inflammatory, antidiabetic, antimicrobial, and anticancer activities (24).
Valeriana officinalis: Valeriana officinalis is a perennial herb of Capriofoliaceae family and has been used as traditional Chinese medicine for years (26). It is locally known as sugandhabala, mushkbala, valerian root and widely found in Europe, Asia and North America (27, 28). The roots and rhizomes of V. officinalis are aromatic with slightly bitter taste and reported to be used in the treatment of insomnia, depression, anxiety and nervous system disorders (Figure 3). V. officinalis is approved by USFDA to be used as dietary supplement in order to improve sleep quality (29). Studies have reported that the essential oil of V. officinalis increases the release of interleukin-1β [IL-1β] and tumor necrosis factor-α [TNF-α], which relaxes the cerebral cortex and has a calming effect. Additionally, other phytochemicals that cause sleep by activating GABA receptors include flavonoids, valerianone, and valerenic acid (26).
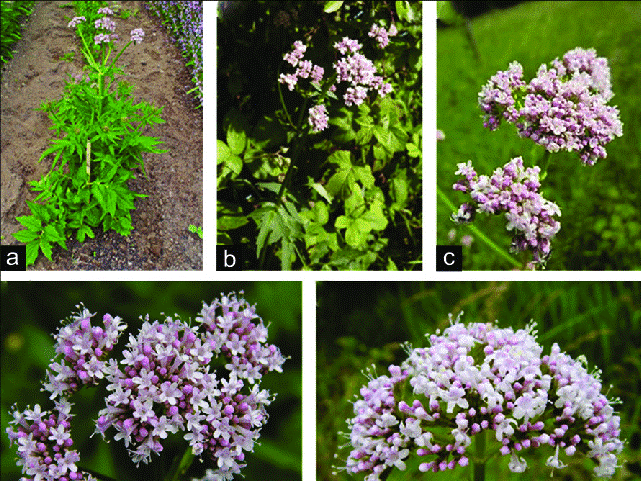
Animal study also revealed that V. officinalis improves behavioral activities in mice by proliferating 5-HT level, hippocampal neurons, and expression of phosphorylated cAMP responsive element binding protein. Hence, their use as anxiolytic and antidepressant has become widespread, with valerenic acid serving as the primary constituent for these effects (31).
Ferula asafoetida: Ferula asafoetida is a herbaceous plant belonging to the Umbelliferae family and is known for its diverse biological and therapeutic properties (Figure 4) (32). It is commonly known as hing, stinging gum, Devil’s drug, ferula, God’s food in local market and generally used in curries, sauces and pickles (33). Traditionally, asafoetida, an oleo-gum-resin derived from the root exudates of Ferula assafoetida, has been used to treat intestinal parasites, gastrointestinal disorders, and asthma. Typically, asafoetida is prepared from Ferula species native to the southern and eastern regions of Iran (34). The major constituents of F. asafetida include ferulic acid, monoterpenes, coumarins, sesquiterpene, sulfur-containing compounds, and polyphenols which are considered responsible for its psychoactive properties. (32).
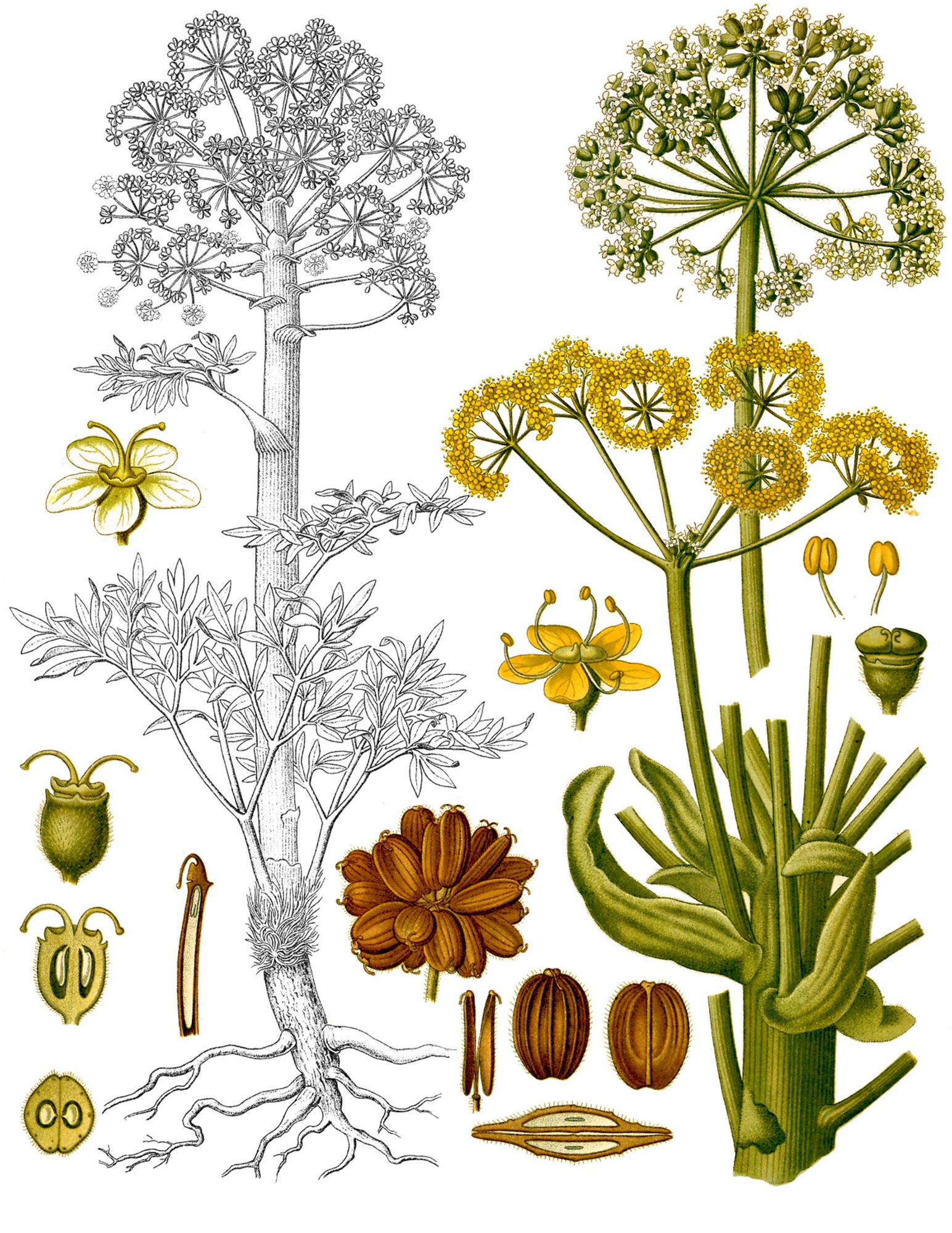
It possesses antidepressant and neuroprotective activities, along with this antispasmodic, antimicrobial, antiviral, antifungal, cancer chemopreventive, anti-diabetic, anti-hypertensive, anticarcinogenic, antimicrobial, and relaxant properties (36–38). In vivo studies have suggested that Ferula exert their pharmacological effect by increasing the levels of serotonine, noradrenaline, and dopamine. These findings suggest that Ferula species have potential as an anxiolytic and sedative agent and may serve as a potential alternative to diazepam. However, further preclinical and clinical studies are required to confirm its efficacy and safety (39, 40).
Cannabis sativa: Cannabis sativa is one species in the genus Cannabinaceae. There are numerous common names for this plant species, and many people call it as hemp or marijuana (Figure 5). Although this plant is native to Central Asia, it has spread throughout the world due to its ability to adapt to several environments.

Numerous bioactive substances are often extracted from cannabis. These substances are classified as alkaloids, carotenoid, flavonoid, lignanamide, terpenoid, stilbenoid, and cannabinoid. The primary component of cannabis, Δ-9-tetrahydrocannabinol (THC), is mainly responsible for its psychoactive effects (41). In addition, cannabidiol (CBD) has been reported to exhibit therapeutic potential in the management of schizophrenia, depression, anxiety, and other neurological disorders (42). THC stimulate the cannabinoid receptors (CB1, CB2) of the brain, increase dopamine release, followed by psychoactive effect. In contrast, CBD interacts with serotonin (5-HT1A) receptors and mediate anxiolytic, antidepressant and panicolytic effect by increasing serotonin release (43). Cannabinoids can be beneficial for a variety of additional diseases, such as Tourette syndrome, PTSD, and sleep issues. It has also anti-inflammatory, anti-cancer, neuroprotective, antifungal, anticoagulant, antibacterial, anti-aflatoxigenic, insecticidal, antioxidant and dermocosmetic properties. Cannabis seeds are used as an analgesic, anxiolytic, antiepileptic, antiemetic, and to treat neurological discomfort (41, 44, 45).
Panax ginseng: Panax ginseng or ginseng, is one of the most significant herbal medicines in Asia belongs to the Araliaceae family of plants. Ginseng roots are widely used in oriental and traditional medicine from ancient days due to its numerous health benefits (Figure 6). It contains a variety of bioactive monomers, including triterpene saponins, fatty acids, polysaccharides, and mineral oils. The triterpene saponins, also referred to as ginsenosides, are the main component responsible for the psychoactive property of ginseng (46–48).

Studies have reported that ginsenoside increases the expression and activity of brain-derived neurotropic factor (BDNF) and phosphorylates extracellular signal-related kinases (ERK) to produce an antidepressant effect. Additionally, ginseng saponin acts on the serotonin receptor (5-HT2A) to boost serotonin production, which improves depression-like behavior (50). Panax ginseng also possesses anti-inflammatory, antioxidant, and anti-apoptotic properties which contribute to their neuroprotective effects on the central nervous system (51).
Papaver somniferum:Opium poppy is one of the world’s oldest medicinal plants (Figure 7). One species that is well known for its variety of alkaloids is Papaver somniferum L. (Family: Papaveraceae). It is typically found in America, Asia, North Africa, and Europe. Since ancient times, it has been used as a strong analgesic and antitussive to treat mild to severe pain (52).
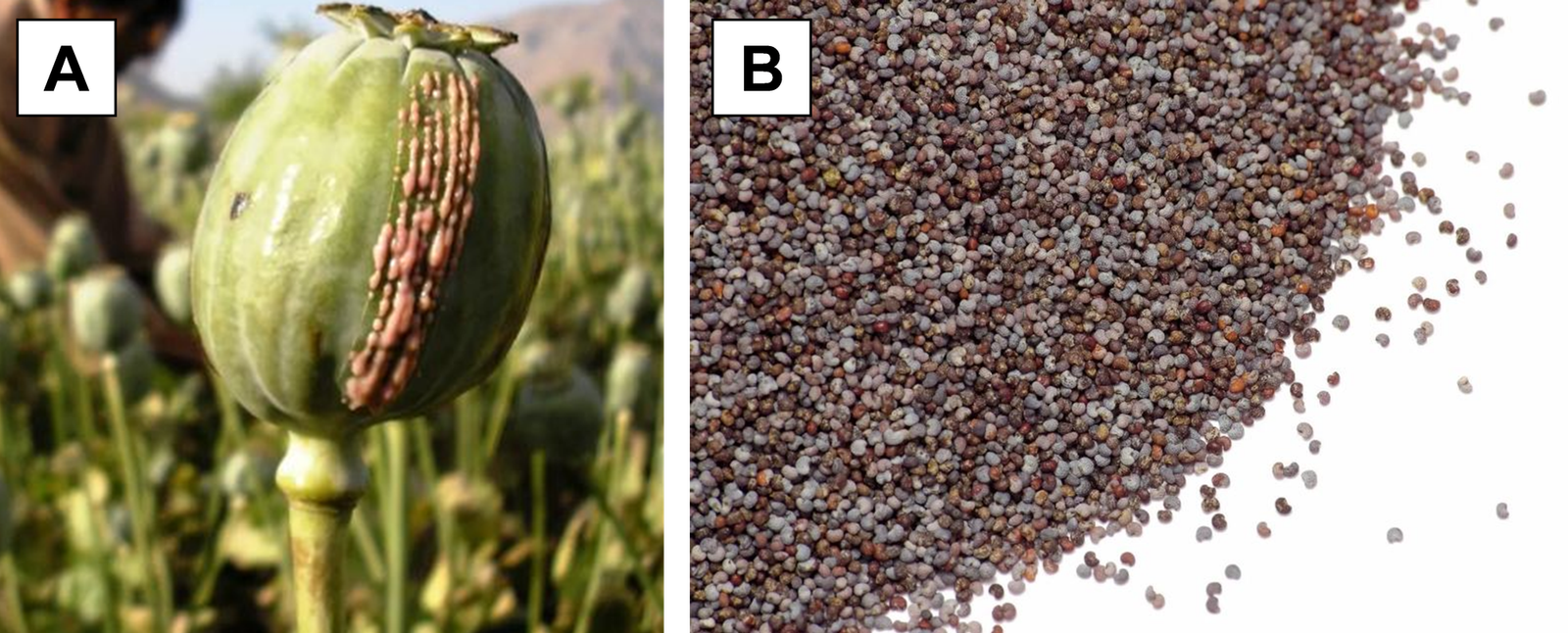
Opioids, the primary component of opium, modify the brain's molecular and neurological pathways, which in turn affects the brain's reward system. Opioid use causes neurological responses and can alter the brain's affective and pain systems, increasing the likelihood of compulsive drug-seeking behavior and causing hypersensitivity. Chronic opioid consumption changes the brain's composition and capabilities, particularly in regions linked to reward, motivation, and judgment. These alterations may have an impact on neurotransmitter systems and neural circuitry, which may impair cognition and raise the danger to one’s mental health conditions like depression and anxiety. Moreover, it may have important psychological implications including altered mood and behavior (52, 54).
Glycerrhiza glabra: The plant Glycyrrhiza glabra, commonly known as licorice, is a member of the Leguminosae family and abundant in the Middle East, Asia, and Europe (Figure 8) (55).

This plant contains more than 400 phytochemical elements including triterpenoid saponins, flavonoids, coumarin, phenolic compounds, pterocarpin etc. Among all the bioactive constituents, licorice total flavonoids (LF) and liquiritine are the prime components with antidepressant activity. Licorice has been shown in studies to have psychoactive properties through a variety of ways. LF and liquiritine reduce serum corticosterone levels and also increase BDNF expression, which causes autophosphorylation of tyrosine kinase B (TrkB) and has an antidepressant effect (57, 58). Additionally, licorice has other therapeutic advantages like sedative, anticoagulant, anti-inflammatory, anti-microbial, anti-asthmatic, anti-cancer, anti-atherogenic, and antispasmodic properties. (55, 59).
Humulus lupulus:Humulus lupulus L. , also known as Hops is a climbing herbaceous perennial from the Cannabaceae family, and extensively used worldwide for fermentation (Figure 9). Although H. lupulus originated in central Europe, it is now widely grown industrially in the North's temperate zones (60).

Phytochemical screening results showed that H. lupulus extract contains 1% volatile oil, 15-25% resins, 2-4% tannins, flavonoids, xanthohumol, ferulic acid, polyphenols, glycosides etc. The oils and resins together is known as lupulin which is responsible for several pharmacological activities (62). Beside several therapeutic effects, recent studies have found the efficacy of hops extract in anxiety, sleep disturbances, depression, ADHD and restlessness. The suggestive mechanism is interaction of lupulin with serotonin receptor (5-HT6) leading to anxiolytic and antidepressant activity. In vivo study also confirmed the sedative and hypnotic effect of hops as they increase the level of γ-aminobutyric acid (GABA) neurotransmitter and relaxes CNS stimulation. Hence, hops are used for the treatment of insomnia alone or in combination with other herbs like valerian (60, 62–65).
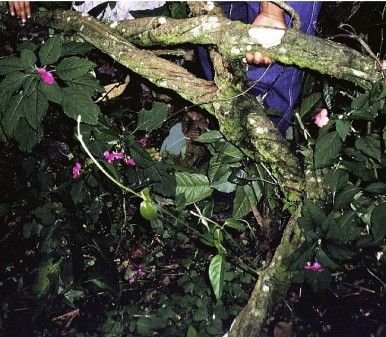
Tabernanthe iboga: Tabernanthe iboga, a plant native to West Africa, contains ibogaine, an indole alkaloid with hallucinogenic properties found in its root bark (Figure 10). This species belongs to the Apocynaceae family, was first classified about 140 years ago (66). The root bark contains about 6% indole alkaloids, including ibogaine, ibogaline, ibogamine, and tabernanthine. Among these, ibogaine makes up roughly 80%, ibogaline 15%, and ibogamine 5%. Ibogaine is a type of tryptamine (67, 68). Its effects are complex, as it influences multiple neurotransmitter systems simultaneously. It shows significant binding to NMDA, kappa-opioid, sigma, and nicotinic receptors. Its interaction with the kappa-opioid receptor likely plays a role in its psychoactive properties (69). Ibogaine's hallucinogenic properties may be due to its modest agonist effect on the serotonin 5HT2A receptor. In addition to reducing dopamine levels, ibogaine accelerates dopamine breakdown (70). It may also reverse opioid-induced changes in gene expression, helping restore normal receptor function and bringing the brain back to a pre-addiction state. Moreover, it appears to interrupt and reset addiction-related brain circuits (66).
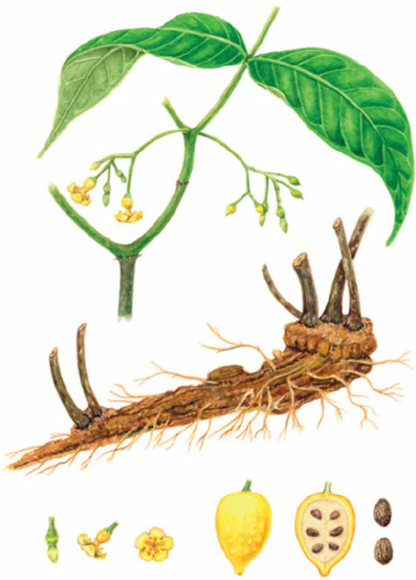
Ibogaine induces vivid, fast-paced visual hallucinations, especially in the dark, along with symptoms like drowsiness, sound sensitivity, insomnia, and physical effects such as dry mouth, sweating, dilated pupils, and tremors. It frequently improves memory recall and self-reflection, allowing individuals to critically examine their thoughts and life experiences. Heroin addicts treated with ibogaine claimed relief from withdrawal and acquired insight into the psychological causes of their addiction, allowing them to build a stronger sense of self (72).
Psilocybe cubensis: For millennia, humans have recognized and intentionally utilized the hallucinogenic properties of certain plants and fungi, among which mushrooms being a primary source for such effect. The magic mushroom, or Psilocybe cubensis, contain psilocybin, a hallucinogenic substance that has long been used in religious and spiritual rites as well as the treatment of neuropsychiatric illnesses (Figure 11) (73, 74).

Major phytochemical constituents of magic mushroom are hydroxylated derivatives of tryptamine, which include psilocybin, psilocin, baeocystin, and norbaeocystin. These days, psilocybin's therapeutic uses are transforming mental health care and providing fresh hope for illnesses including depression, PTSD, and terminal anxiety. The two main active ingredients that provide the psychoactive effects are psilocybin (O-phosphoryl-4-hydroxy-N, N-dimethyltryptamine) and psilocin (4-hydroxy-N, N-dimethyltryptamine) (73, 74, 76–79). It is suggested that psilocybin affects serotonergic system (5-HT) as a non-selective agonist of 5-HT2A followed by therapeutic efficacy against several neuropsychiatric disorders like anxiety, depression, OCD, addiction etc. (80).
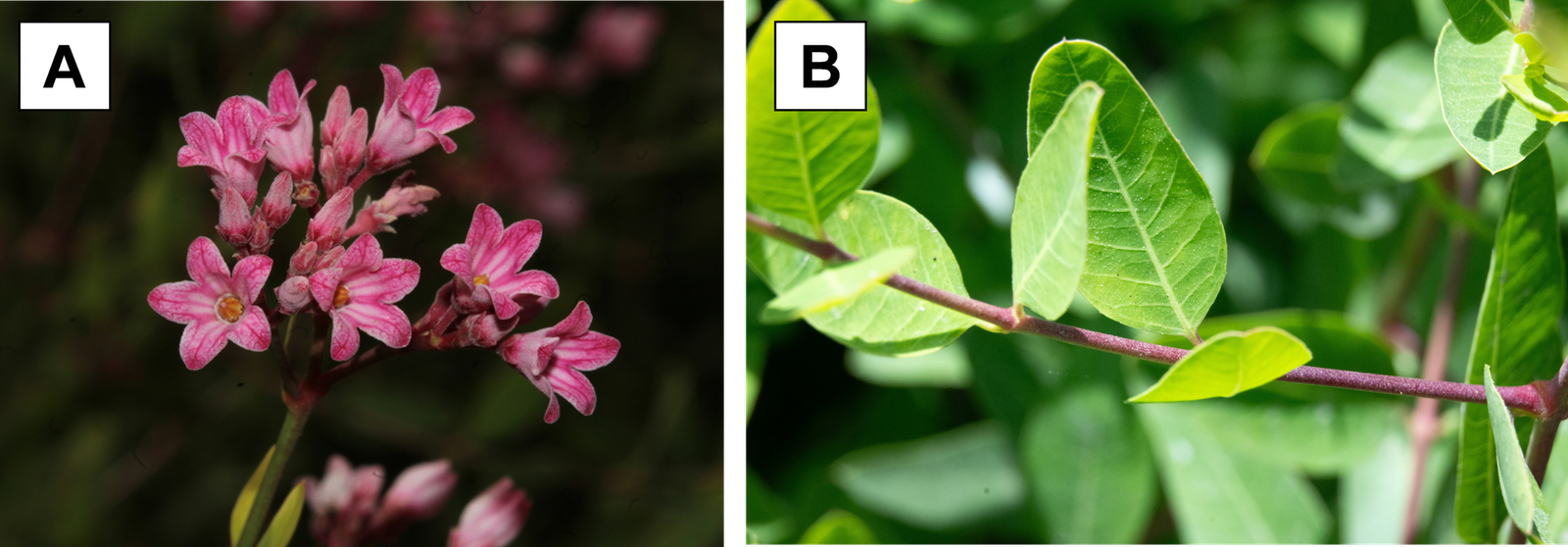
Banisteriopsis caapi: Banisteriopsis caapi is a psychoactive plant vine of the Malpighiaceae family, native to Amazon rainforest (Figure 12). It is also known as cappi, yage, soul vine and found as the core ingredient of psychoactive decoction, Ayahuasca (81). The antidepressant activity of cappi has been reported in both animal studies and clinical trials. B. caapi mainly contains β-carboline indole alkaloids namely harmine, tetrahydroharmine, and harmaline along with some polyphenols. Alkaloids present in cappi reversibly inhibit monoamine oxidase A (MAO-A) enzyme followed by reduced degradation of serotonin, noradrenaline and dopamine and results in psychoactive effect. Similarly, tetrahydroharmine also inhibits the reuptake of serotonin by 5-HT2A and ensures the anxiolytic and antidepressant effect. Moreover, β-carboline alkaloids stimulate neurogenesis by increasing the BDNF in hippocampal region that also helps in improvement of depressive behaviors (82, 83).
Psychotria viridis: Psychotria viridis, locally known as chacrona, rainha, belongs to the coffee family Rubiaceae, is a perennial shrubby flowering plant (Figure 13). It has been used in a common version ofAyahuasca tea with Banisteriopsis cappi (84). P. viridis leaves contain serotonin like alkaloid, N, N-Dimethyltriptamine (DMT) which is responsible for the psychoactive effect revealed by the activation of 5-HT2A receptors.

Additionally, DMT also interacts with sigma-1 intracellular receptors which plays important role in producing antidepressant and antipsychotic effects (86). Beside the psychoactive properties, P. viridis also possesses other pharmacological benefits like anti-inflammatory, antibacterial, antioxidant, analgesic properties (87-89).
Salvia officinalis: The plant Salvia officinalis, also known as Sage, belongs to the Labiatae/Lamiaceae family. It is an evergreen, perennial subshrub with woody stem and grayish leaves (Figure 14). Although it originated in the Middle East and the Mediterranean, it has now spread around the world. This aromatic plant is frequently used in tea along with its use in Asian and Latin American traditional medicine to treat a variety of conditions such as seizures, ulcers, gout, rheumatism, inflammation, disorientation, tremor, paralysis, diarrhea, and hyperglycemia. S. officinalis has been used in European traditional medicine to treat age related cognitive problems, excessive perspiration, mild dyspepsia (including heartburn and bloating), and skin and throat inflammations (90, 91).

Numerous terpenes and phenolics present in sage (Salvia) plants interact with brain function-related processes, improving certain aspects of cognitive performance. The principal ingredients are alkaloids, phenolic chemicals (e. g., coumarine), flavonoids (e. g., chlorogenic acid, rosamarinic acid, caffeic acid), carbohydrates (e. g., arabinose, galactose, mannose), terpenoids, steroids, and so on. The volatile oil derived from sage are rich in flavonoids such as borneol, camphor, linalool, cineole, humulene, thujone, pinene, limonene (91). Animal studies support the anxiolytic and antidepressant effects of sage leaf extracts, as well as the improvement of cognitive behavior. According to research, sage, which is rich in flavonoids and essential oils, may operate as a psychoactive agent in the treatment of anxiety, depression, and behavioral problems (93).
Apocynum venetum: Apocynum venetum is a perennial herbaceous shrub from the family Apocynaceae (Figure 15). It is referred to as "Luobuma" in Chinese and "Rafuma" in Japanese and has been used as food supplement for its numerous medicinal values (94). The primary constituents of the shrub include flavonoids (apocynins A–D, quercetin, hyperin, lupeol, scopoletin isofraxidin, and kaempferol), phenols, and beta-sitosterol. The presence of several flavonols, flavanols, and glycosides in this plant can account for a range of pharmacological activities, such as antihypertensive, hepatoprotective, hypnotic, depressive, anxiolytic, and antioxidant properties (95).
In addition, it can be used to treat major depression with efficacy comparable to tricyclic antidepressants. In vivo experiments showed that A. venetum extracts relief the symptoms of major depressive disorder (MDD), including persistent melancholy, disinterest, loss of enjoyment, low self-esteem, difficulty concentrating, feelings of guilt or exhaustion, and irregular eating or sleeping patterns (94-97).
Hypericum perforatum: Hypericum perforatum (Family: Hypericaceae), known as Saint John's wort (SJW), is a perennial herb indigenous to northern Africa, western Asia, and Europe (Figure 16). It was originally applied in a variety of traditional medicinal systems, such as, Islamic, Greek, and Chinese medicine. St. John's Wort is used as an over-the-counter anxiolytic or antidepressant (98).

It is a xenobiotic made up at least 10 groups of physiologically active, identifiable chemicals, including flavonoids, campferol, rutin, hyperoside, and quercetin and five different types of hypericin. According to reports, St. John's Wort functions as a reuptake inhibitor of serotonin, dopamine, and norepinephrine, which is one of the primary processes utilized in healthcare. This reduces the uptake of dopamine, norepinephrine, and serotonin at neural synapses. Increased neurotransmitter levels are thought to be beneficial in the treatment of depression. Besides, the ability to bind to GABA receptors and reduce GABA binding, which lowers CNS depression (99, 100).
Additionally, this plant has a variety of therapeutic applications, including as antibacterial, antidepressant, neuroprotective, anxiolytic. St. John's wort has also been used to treat psoriasis, obsessive-compulsive disorder, behavioral problems, and menopausal somatic symptoms (98, 99, 101).
Passiflora incarnata: Passiflora incarnata, often known as Passion flower, is a member of the Passifloraceae family (Figure 17). The species is indigenous to Australia, South East Asia, and South America. Since ancient times, Passiflora-based herbal remedies have been used extensively to treat anxiety (102).

The plant's fruits, flowers, and aerial portions are all utilized medicinally. Passiflora incarnata contains flavonoids, cyanogenic glycosides, alkaloids, and phenolic compounds. The primary phytochemicals found in passionflower are flavonoids (kaempferol, quercetin, luteolin, and apigenin), alkaloids (hamaline, harmalol, harmine, harmol), coumarine, phytosterols and glycosides (vitexin, isovixetin, orientin) (104, 105). On the other hand, passion fruits are rich in phenols, carotenoids, flavonoids and tannins while the leaves contain flavonoids and tanins mainly with slight amount of alkaloids (106, 107). Owing to the rich content of flavonoids, P. incaranata is widely used as herbal supplement for the ailment of anxiety, insomnia, seizures, hysteria etc. It has also been reported to exhibit therapeutic potential in the management of morphine dependence, insomnia, neurotic disorders, and attention-deficit/hyperactivity disorder (ADHD) (104, 108). Usually, pharmacological actions of P. incarnate are mediated via GABA system regulation, which includes GABAA and GABAB receptor affinity as well as effects on GABA absorption. Consequently, GABAA system involvement has anxiolytic effects (104, 109, 110).
Withania somnifera: Withania somnifera, also known as Ashawagandha is a plant of Solanaceae family which is highly renowned for its medicinal values (Figure 18). Ashwagandha has long been used as an adaptogen in ancient Ayurvedic and Unani medical systems. Herbs known as adaptogens enhance the body's reactions to stress and aid in adaptation by restoring physiological functions during periods of elevated stress. Adaptogens exert their stress-protective effect by regulating homeostasis via several mechanisms of action associated with the hypothalamic pituitary adrenal (HPA) axis (111).

Ashwagandha contains acylsterylglucosides and sitoindosides, which have anti-stress properties. It has been shown that ashwagandha's active compounds, such as sitoindosides VII-X and Withaferin-A, have potent anti-stress effects. As a result, Ashwagandha can be used to treat Huntington's disease, Parkinson's disease, Alzheimer's disease, and other neurological disorders at any stage of their progression. Ibotenic acid-induced cognitive deficits in Alzheimer's disease were significantly reversed by glycowithanolides containing aferin-A and sitoindosides VII-X isolated from ashwagandha roots. Furthermore, biologically active chemical components of W. somnifera include alkaloids (Anahygrine, cuseohygrine, anaferine, isopelletierine, and so on), steroidal lactones (withanolides, withaferins), and saponins. Apparently being a multifunctional herb, ashwagandha has anti-inflammatory, neuroprotective, adaptogenic, hematopoietic, memory-enhancing, sleep-inducing, anxiolytic, and antidepressant characteristics (111, 115).
Camellia sinensis: Camellia sinensis belongs to the family Theaceae and known as tea throughout the world (Figure 19). The main growing environments for this tree are tropical and subtropical areas. Teas can be classified depending on the degree of fermentation as green tea (unfermented tea), white tea and yellow tea (lightly fermented), oolong tea (semi-fermented tea), black tea (fermented tea), and pu-erh tea (post-fermented tea). Throughout human history, green tea has been one of the most popular drinks drank worldwide.

The principal bioactive substances found in Camellia sinensis leaves are caffeine, flavonols namely catechin, epigallocatechin gallate (EGCG); glycosyl derivatives including apigenin, myricetin, quercetin; and rutin, teaflavins, and thearubigins. Green tea has long been used to promote relaxation, physical stimulation, mental clarity, and cognitive function. Caffeine, L-theanine, and EGCG have been found to improve mood and cognitive function on numerous occasions. Green tea contains L-theanine, a non-proteinic amino acid that has effects on brain. Regular and frequent tea consumption has been linked to improvements in mood, health, and cognitive function. It has been proven that L-theanine and caffeine improve task performance and attention span. Additionally, L-theanine is believed to boost mood by causing the brain's α-waves to be stimulated. In a brief amount of time, this substance is usually linked to increased energy, motivation, focus, and performance. Hence, it is the most often used as psychoactive stimulant globally (117, 118).
Rhodiola rosea: Rhodiola rosea L. , commonly referred to as "arctic root," "roseroot," or "golden root," is a member of the Crassulaceae family (Figure 20). It is well recognized to strengthen memory and learning, protect the brain, and promote cognitive performance (119).

From R. rosea's roots and rhizome, about 140 compounds have been identified, including proanthocyanidins, flavonoids, flavonlignans, cyanogenic glycosides, aryl glycosides, phenylethanoids, phenylpropanoids, and their glycosides, as well as monoterpene alcohols and their glycosides (121). R. rosea has antidepressant effects through altering defense mechanism proteins (e. g., heat shock proteins Hsp 70 and FoxO/DAF-16), nitric oxide, and protein kinases p-JNK in addition to its interaction with the HPA-system (cortisol-reducing). Certain components of R. rosea raise the levels of 5-HT and noradrenaline in the frontal, prefrontal, and cerebral cortex resulting in improved depression symptoms. It has long been used in traditional medicine to strengthen the nervous system, alleviate depression and stress-induced fatigue, increase longevity, physical performance, and resistance to high altitude sickness, as well as to treat anemia and fatigue. Cardioprotective, antifatigue, anxiolytic, nootropic, life-extending, and central nervous system stimulating effects are some additional medicinal use of R. rosea (122-124).
Avena sativa: Avena sativais a domesticated cereal grass from the family Poaceae and grown primarily for its edible grains (Figure 21). It is usually known as ‘oats’, ‘green oats’ or ‘common oat’. The higher aerial parts of Avena sativa plants are used to make immature or "green" oat extracts and tinctures, which have a long history of medical use and cover a variety of psychoactive indications, such as anxiety and sleeplessness (125).

A variety of possibly beneficial secondary metabolite compounds and multiple categories of potentially psychoactive phytochemicals are often found in green oat (Avena sativa) preparations. These invariably comprise a variety of terpenes, including species-specific triterpene saponins known as "avenacins," a wide range of phenolic acids and polyphenols, some of which include flavonoids and avenanthramides (125). The green oat extracts inhibit the monoamine oxidase B (MAO-B) and phosphodiesterase 4 (PDE-4) enzymes that increase the dopaminergic availability. As dopamine plays a cardinal role in mood improvement, oat extracts could alleviate anxiety, depression and cognition (127). A summary of the major psychoactive constituents of the discussed plants is presented in Table 2.
| No. | Name of the plant | Major psychoactive constituent | Reference |
|---|---|---|---|
| 1. | Myristica fragrans | Myristicin, Myristic acid, Elemicin | (24) |
| 2. | Valeriana officinalis | Valerenic acid, Valerenal, Valerianone | (26) |
| 3. | Ferula asafoetida | Ferulic acid, Coumarine, Monotrpenes, Sequiterpene, Sulphide compounds | (32) |
| 4. | Cannabis sativa | Δ-9-Tetrahydrocannabinol, Terpenoid, Cannabinoid. | (42) |
| 5. | Panax ginseng | Ginsenoside, saponin, fatty acid. | (46) |
| 6. | Papaver somniferum | Opioids, morphin | (54) |
| 7. | Glycyrrhiza glabra | Glycyrrhizin, Glycyrrhetinic acid, Liquiritin, Isoliquiritin, | (58) |
| 8. | Humulus lupulus | Lupulin, Triterpenes, Flavonols, Tannins, Ferulic acid | (128) |
| 9. | Atropa belladonna | Scopolamine, Hyoscyamine, Atropine | (129) |
| 10. | Psilocybe cubensis | 5-methylpsilocybin, Psilocin | (77) |
| 11. | Banisteriopsis caapi | Harmine, Tetrahydroharmine, Harmaline | (82) |
| 12. | Psychotria viridis | N, N-dimethyltryptamine | (87) |
| 13. | Salvia officinalis | α-thujone, 1, 8-cineole, Camphor, Rosamarinic acid | (91) |
| 14. | Apocynum venetum | Quercetin, Apocynins, Phenols, β-sitosterol | (97) |
| 15. | Hypericum perforatum | Hyperforin, Hypericin, Quercetin | (101) |
| 16. | Passiflora incarnata | Harmalol, Kaempferol, Lutionin, Coumarine | (104) |
| 17. | Withania somnifera | Withaferins, sitoindosides | (111) |
| 18. | Camellia sinensis | L-theanine, Caffeine, epigallocatechin gallate | (117) |
| 19. | Rhodiola rosea | Flavanoids, Monoterpenes, Rosiridol | (123) |
| 20. | Avena sativa | Avenacins, Flavonoids, Terpenes | (126) |
The above discussion reveals the emerging scope of using medicinal plants in psychological disorders like anxiety, depression, insomnia, stress, ADHD, PTSD etc. Review data indicate that a number of plants in our surroundings could act as psychoactive agents. Asafoetida, ashwagandha, ginseng, and other medicinal herbs have chemical components that significantly alter mental health conditions. These plants contain bioactive compounds that may serve as potential candidates for future neuropharmacological research. The phytochemical constituents obtained either from the leaves, stem, roots, flowers of the above mentioned plants are particularly flavonoids, alkaloids, phenolic components, resins, terpenes which act on the neurotransmitters. They lead to increased level of serotonin, dopamine, noradrenaline in the brain along with reduced serotonin and dopamine reuptake. Besides, some of the psychoactive agents are able to increase neurogenesis by elevated expression of BDNF in hippocampal region of brain. Preclinical and limited clinical findings suggest that some of these plants may contribute to improvement of depressive symptoms, anxiety, restlessness, sleep quality, cognitive behaviors and mood.
The psychoactive effects of the medicinal plants discussed in this review are mainly associated with diverse phytochemical groups, including alkaloids, flavonoids, terpenoids, cannabinoids, phenolic compounds, and saponins. Several well-known bioactive compounds, such as psilocybin, psilocin, Δ9-tetrahydrocannabinol (THC), cannabidiol (CBD), valerenic acid, ginsenosides, harmine, harmaline, and myristicin, have been reported to interact with neurotransmitter systems involved in central nervous system regulation. These phytochemicals may exert neuropharmacological effects by modulating serotonergic, dopaminergic, GABAergic, monoaminergic, and endocannabinoid signalling pathways. In addition, certain structural features of these compounds, including indole alkaloid structures, phenolic moieties, and lipophilic terpene constituents, may also contribute to their receptor-binding ability and psychoactive activity. However, detailed structure-activity relationship studies and advanced phytochemical characterisation remain limited for many medicinal plants. Summative information on some psychoactive chemicals with possible mechanism of action is presented in Table 3.
| Plant | Major phytochemicals | Proposed neuropharmacological target/mechanism |
|---|---|---|
| Cannabis sativa | Δ9-THC, CBD | CB1/CB2 receptor modulation; serotonergic activity |
| Psilocybe cubensis | Psilocybin, psilocin | 5-HT2A receptor agonistic activity |
| Valeriana officinalis | Valerenic acid, flavonoids | GABAergic modulation |
| Banisteriopsis caapi | Harmine, harmaline | MAO-A inhibition; serotonergic modulation |
| Panax ginseng | Ginsenosides | BDNF regulation; serotonergic signaling |
| Myristica fragrans | Myristicin, elemicin | CNS stimulation and possible serotonergic interaction |
Toxicity and Safety Concerns
Although many psychoactive medicinal plants demonstrate significant neuropharmacological potential, their inappropriate or excessive use may lead to adverse reactions, toxicity, drug interactions, or dependence (130) (see Supplemental Table 1). Safety concerns remain particularly relevant for plants containing potent hallucinogenic or opioid-like compounds because of their strong psychoactive effects and potential for misuse. Papaver somniferum may cause respiratory suppression, tolerance development, and opioid dependence due to the presence of morphine-derived alkaloids. Atropa belladonna contains tropane alkaloids that may may cause lethargy, coma, and potentially fatal outcomes.
Excessive consumption of Cannabis sativa has been linked to impaired cognition, anxiety, dependency, and neurochemical imbalance, temporary reduction in motor activity in susceptible individuals. Similarly, uncontrolled use of Psilocybe cubensis or plants used in ayahuasca preparations may trigger intense psychological disturbances, altered perception, and unfavorable psychiatric effects. In addition, some medicinal plants can interfere with conventional medications by affecting hepatic enzyme activity or neurotransmitter systems (131). The regulatory status and toxic effects of plants listed in highlight the need for cautious use, as several of these species are associated with significant safety concerns. Consequently, proper dose standardization, toxicological assessment, and professional medical guidance are critical to ensure their safe therapeutic application.
Pharmacokinetics and Dosage Considerations
The pharmacokinetic properties, bioavailability, metabolic pathways, and dose-dependent effects of numerous plant-derived psychoactive compounds have not yet been adequately investigated (132). Differences in geographical origin, cultivation conditions, extraction techniques, preparation processes, and phytochemical composition can substantially affect both therapeutic effectiveness and safety profiles. Moreover, variability in dosage practices and the scarcity of long-term toxicity studies make it difficult to establish reliable and standardized clinical applications (133).
Some psychoactive medicinal plants may also interact with conventional pharmaceutical agents through alterations in neurotransmitter signalling pathways or hepatic enzyme activity, potentially increasing the likelihood of adverse effects, contraindications, and drug interactions. Consequently, further pharmacokinetic, toxicological, and well-designed clinical investigations are necessary to support the safe, effective, and reproducible therapeutic use of these plant-derived compounds.
Evidence Level and Clinical Translation
The strength of scientific evidence varied substantially among the medicinal plants included in this review. Some plants, such as Cannabis sativa, Psilocybe cubensis, and Withania somnifera, have relatively stronger experimental support along with limited clinical evidence demonstrating their neuropharmacological potential (134). In contrast, many other plants are still supported mainly by ethnopharmacological knowledge, traditional therapeutic practices, and preliminary in vitro or animal-based investigations. Although a wide range of phytochemicals exhibited promising psychoactive and neuroactive mechanisms, the translation of preclinical outcomes into validated clinical efficacy remains restricted. This limitation is largely associated with the scarcity of well-controlled human studies, absence of standardized formulations, and significant variability in dosage, extraction methods, and phytochemical composition. Consequently, interpretation of therapeutic effectiveness should be approached cautiously until further more rigorous and well-designed clinical evidence becomes available.
Ethical and Regulatory Considerations
The therapeutic use of psychoactive medicinal plants involves important ethical and regulatory issues. Many of the plants discussed in this review are controlled or restricted in various countries due to their psychoactive properties, potential for misuse, and risk of dependence. Regulations related to medicinal Cannabis sativa, psilocybin-containing fungi such as Psilocybe cubensis, opioid-bearing plants, and ayahuasca preparations differ widely across different legal and healthcare frameworks (135). Ethical challenges, including recreational misuse, self-medication without supervision, dependence, and non-medical consumption, remain key concerns in both research and clinical contexts. Therefore, future advancement of psychoactive medicinal plants in therapeutic settings requires strict regulatory control, standardized pharmaceutical formulations, precise dose regulation, and well-designed clinical trials to ensure safety, efficacy, and responsible application in healthcare.
Future Prospects of Medicinal Plants Use in Mental Health Disorders
Medicinal plants continue to attract considerable scientific interest as potential sources of novel neuropharmacological agents for the management of mental and neurological disorders. Increasing evidence suggests that plant-derived phytochemicals may provide therapeutic benefits through modulation of neurotransmitter systems, neuroinflammatory pathways, oxidative stress, and neurogenesis. Advances in phytochemistry, molecular pharmacology, and biotechnology may facilitate the isolation, characterization, and development of safer and more effective plant-derived psychoactive compounds for future therapeutic applications. Ancient civilizations, including those in India, China, South America, and Egypt, continue to rely on plant-based remedies for these conditions (72). The World Health Organization (WHO) reports that 60% of the global population uses medicinal plants, with 80% of people in developing countries depending on them for primary healthcare (136). Phytocompounds and their chemical analogs have led to the development of clinically useful drugs for treating both chronic and acute diseases. For centuries, medicinal plants have been widely practiced as treatments, particularly for common ailments like colds, allergies, upset stomachs, and toothaches. Despite a decline in their use within conventional medical practices in the mid-20th century, the interest in natural remedies continues to grow. Throughout history, various medicinal and psychoactive plants have played significant roles in healing, spirituality, and cultural rituals (137-139). The opium poppy has been widely used as a narcotic analgesic for pain relief. Cannabis, also known as marijuana, was commonly utilized by shamans for its mild hallucinogenic effects, often revealing subconscious thoughts and triggering memories. Wormwood, an ancient hallucinogenic herb, was a key ingredient in absinthe, a drink that was later banned in the 20th century due to its psychoactive properties. The peyote cactus, containing mescaline, has been used in indigenous rituals for its powerful visual and mystical hallucinations. In Africa, the Bwiti cult consumed iboga, a hallucinogen believed to facilitate communication with ancestral spirits. Meanwhile, in the Amazon, indigenous tribes in Peru, Bolivia, and Brazil prepared ayahuasca, a potent psychoactive brew containing DMT and MAO inhibitors, which was central to religious and spiritual enlightenment ceremonies. These plants have long been intertwined with medicine, mysticism, and cultural traditions, shaping human history through their profound effects on consciousness (72). However, in recent years, the WHO has emphasized the importance of documenting the use of medicinal plants by these traditional practitioners. This has led to efforts in developing countries to record ethnomedical knowledge about plants, making it easier to scientifically validate their pharmacological properties. Once these local plant preparations are properly evaluated and disseminated, people will be more informed and confident in using effective treatments, which may contribute to improved healthcare understanding and future therapeutic research (136). Future investigations involving advanced phytochemical characterization, metabolomic profiling, and structure-activity relationship studies may further improve clearer understanding of the neuroactive properties of medicinal plant constituents.
Limitations of the Review
Several limitations need to be acknowledged when interpreting the results of this review. A large proportion of the existing evidence on psychoactive medicinal plants is derived from preclinical experiments, in vitro studies, or ethnopharmacological reports, while rigorously designed clinical trials remain scarce. In addition, marked variability is observed across studies in terms of experimental design, extraction procedures, phytochemical profiles, administered doses, and measured outcomes, which complicates meaningful comparison of results. Differences in plant source, processing techniques, and concentrations of active constituents may further contribute to inconsistencies in both pharmacological effects and safety outcomes. Moreover, legal restrictions and ethical constraints surrounding certain psychoactive species also hinder extensive clinical research. In addition, the broad narrative approach of this review and the diversity of the available evidence may limit direct comparisons between studies and make it difficult to draw definitive conclusions regarding clinical efficacy and safety. Accordingly, there is a strong need for future studies employing standardized methodologies and well-controlled clinical designs to better establish efficacy, safety, optimal dosing, and long-term therapeutic potential.
Conclusion
Medicinal plants are a valuable source of biologically active compounds that may exert psychoactive and neuropharmacological effects. The plants discussed in this review contain a wide range of phytochemical classes, including alkaloids, flavonoids, cannabinoids, terpenoids, phenolic compounds, and saponins, which can modulate central nervous system activity through different neurochemical mechanisms. A number of these plants have shown anxiolytic, antidepressant, sedative, hallucinogenic, cognitive-enhancing, and neuroprotective properties in preclinical research, with only limited support from clinical studies. Despite promising therapeutic potential, current evidence remains insufficient to establish these medicinal plants as direct alternatives to conventional psychoactive medications. Major limitations include the lack of standardized formulations, inconsistency in phytochemical content, limited human clinical trials, potential toxic effects, and inadequate long-term safety data. As a result, future research should prioritize on well-standardized pharmacological investigations, rigorous clinical trials, comprehensive toxicity assessments, and clear regulatory frameworks to support the safe and evidence-based therapeutic applications of psychoactive medicinal plants.
Declarations
Conflict of Interest
The authors declare no conflicting interest.
Data Availability
The data generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
Ethical approval was not required for this study.
Funding Information
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Table 1 is available as supplementary material at the journal's website (<a class="cursor-pointer" href="https://etflin.com/file/document/20260521172733_799249_7afd35d4.docx">link</a>).
References
- Galson SK. Mental Health Matters. Public Health Rep. 2009;124(2):189-191. doi: https://doi.org/10.1177/003335490912400202
- Guthold R, Carvajal-Velez L, Adebayo E, Azzopardi P, Baltag V, Dastgiri S, et al. The Importance of Mental Health Measurement to Improve Global Adolescent Health. Journal of Adolescent Health. 2023;72(1):S3-S6. doi: https://doi.org/10.1016/j.jadohealth.2021.03.030
- Stein DJ, Palk AC, Kendler KS. What is a mental disorder? An exemplar-focused approach. Psychol. Med. 2021;51(6):894-901. doi: https://doi.org/10.1017/s0033291721001185
- National Collaborating Centre for Mental Health (UK). Common Mental Health Disorders: Identification and Pathways to Care [Internet]. Leicester (UK): British Psychological Society (UK); 2011 [cited 2025 Jun 16]. (National Institute for Health and Care Excellence: Guidelines). Available from: http://www.ncbi.nlm.nih.gov/books/NBK92266/ PubMed PMID: 22536621.
- Mental Illness - National Institute of Mental Health (NIMH) [Internet]. [cited 2026 Apr 26]. Available from: https://www.nimh.nih.gov/health/statistics/mental-illness
- Müller CP, Homberg JR. The role of serotonin in drug use and addiction. Behav Brain Res. 2015 Jan 15;Special Issue: Serotonin277:146–92. doi:10.1016/j.bbr.2014.04.007
- WHO. Mental disorders [Internet]. 2022 [cited 2024 Sep 11]. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-disorders
- Seifert R, Schirmer B. A simple mechanistic terminology of psychoactive drugs: a proposal. Naunyn-Schmiedeberg's Arch Pharmacol. 2020;393(8):1331-1339. doi: https://doi.org/10.1007/s00210-020-01918-x
- Siddique N, Hussain S, Yadav S, Gupta A. Psychosis and antipsychotic plants an: overview. Int J Indig Herb Drug. 2022:22-29. doi: https://doi.org/10.46956/ijihd.v7i1.286
- Gahalawat M, Gahalawat P, Kumar K. Application of medicinal plants in mental health care: a comprehensive review. Ijar. 2024;12(07):754-757. doi: https://doi.org/10.21474/ijar01/19108
- Kennedy DO. Phytochemicals for Improving Aspects of Cognitive Function and Psychological State Potentially Relevant to Sports Performance. Sports Med. 2019;49(S1):39-58. doi: https://doi.org/10.1007/s40279-018-1007-0
- Salem MA, Zayed A, Ezzat SM. Psychoactive plants and phytochemicals. Elsevier; 2021. doi: https://doi.org/10.1016/b978-0-12-821556-2.00028-1
- Pantano F, Graziano S, Pacifici R, Busardò FP, Pichini S. New Psychoactive Substances: A Matter of Time. Cn. 2019;17(9):818-822. doi: https://doi.org/10.2174/1570159x1709190729101751
- Schifano F, Napoletano F, Chiappini S, Guirguis A, Corkery JM, Bonaccorso S, et al. New/emerging psychoactive substances and associated psychopathological consequences. Psychol. Med. 2019;51(1):30-42. doi: https://doi.org/10.1017/s0033291719001727
- Jamieson CS, Misa J, Tang Y, Billingsley JM. Biosynthesis and synthetic biology of psychoactive natural products. Chem. Soc. Rev. 2021;50(12):6950-7008. doi: https://doi.org/10.1039/d1cs00065a
- Nichols DE. Psychedelics. Pharmacological Reviews. 2016;68(2):264-355. doi: https://doi.org/10.1124/pr.115.011478
- O’Neill-Dee C, Spiller HA, Casavant MJ, Kistamgari S, Chounthirath T, Smith GA. Natural psychoactive substance-related exposures reported to United States poison control centers, 2000–2017. Clinical Toxicology. 2019;58(8):813-820. doi: https://doi.org/10.1080/15563650.2019.1688341
- Coimbra N, Mendes-Gomes J, da Silva J, dos Anjos-Garcia T, Ullah F, Almada R. New Ethological and Morphological Perspectives for the Investigation of Panicolytic-Like Effects of Cannabidiol. Elsevier; 2017. doi: https://doi.org/10.1016/b978-0-12-800756-3.00098-3
- Muñoz E, Pollastro F, Taglialatela-Scafati O, Appendino G. Peroxisome Proliferator Activated Receptors and Cannabinoids. Elsevier; 2017. doi: https://doi.org/10.1016/b978-0-12-800756-3.00080-6
- WHO. Opioid overdose [Internet]. 2023 [cited 2025 Mar 8]. Available from: https://www.who.int/news-room/fact-sheets/detail/opioid-overdose
- Gupta PK. Chapter 24 - Drug toxicity, dependence, and abuse. In: Gupta PK, editor. Fundamentals of Toxicology [Internet]. Academic Press; 2016 [cited 2025 Mar 13]. p. 277–85. Available from: https://www.sciencedirect.com/science/article/pii/B978012805426000024X doi:10.1016/B978-0-12-805426-0.00024-X
- Ashokkumar K, Simal‐Gandara J, Murugan M, Dhanya MK, Pandian A. Nutmeg (Myristica fragrans Houtt.) essential oil: A review on its composition, biological, and pharmacological activities. Phytotherapy Research. 2022;36(7):2839-2851. doi: https://doi.org/10.1002/ptr.7491
- Al-Rawi SS, Ibrahim AH, Ahmed HJ, Khudhur ZO. Therapeutic, and pharmacological prospects of nutmeg seed: A comprehensive review for novel drug potential insights. Saudi Pharmaceutical Journal. 2024;32(6):102067. doi: https://doi.org/10.1016/j.jsps.2024.102067
- Sultan MT, Saeed F, Raza H, Ilyas A, Sadiq F, Musarrat A, et al. Nutritional and therapeutic potential of nutmeg ( Myristica fragrans ): A concurrent review. Cogent Food & Agriculture. 2023;9(2). doi: https://doi.org/10.1080/23311932.2023.2279701
- El-Alfy AT, Joseph S, Brahmbhatt A, Akati S, Abourashed EA. Indirect modulation of the endocannabinoid system by specific fractions of nutmeg total extract. Pharmaceutical Biology. 2016;54(12):2933-2938. doi: https://doi.org/10.1080/13880209.2016.1194864
- Li J, Li X, Wang C, Zhang M, Ye M, Wang Q. The potential of Valeriana as a traditional Chinese medicine: traditional clinical applications, bioactivities, and phytochemistry. Front. Pharmacol. 2022;13. doi: https://doi.org/10.3389/fphar.2022.973138
- Bhardwaj P, Rattan S, Naryal A, Bhardwaj A, Warghat AR. Valeriana jatamansi. Elsevier; 2021. doi: https://doi.org/10.1016/b978-0-12-823151-7.00013-1
- Das G, Shin HS, Tundis R, Gonçalves S, Tantengco OAG, Campos MG, et al. Plant Species of Sub-Family Valerianaceae—A Review on Its Effect on the Central Nervous System. Plants. 2021;10(5):846. doi: https://doi.org/10.3390/plants10050846
- He B, Chen Y, Yu S, Hao Y, Wang F, Qu L. Food plant extracts for sleep-related skin health: Mechanisms and prospects. Food Bioscience. 2022;49:101951. doi: https://doi.org/10.1016/j.fbio.2022.101951
- Nandhini S, Narayanan KB, Ilango K. Valeriana officinalis: a review of its traditional uses, phytochemistry and pharmacology. Asian J Pharm Clin Res. 2018;11(1):36. doi: https://doi.org/10.22159/ajpcr.2017.v11i1.22588
- Tang J. Effects of Valerian on the level of 5-hydroxytryptamine, cell proliferation and neurons in cerebral hippocampus of rats with depression induced by chronic mild stress. J Chin Integr Med. 2008;6(3):283-288. doi: https://doi.org/10.3736/jcim20080313
- Mahmoud AM, Alruhaimi RS, Hassanein EH. Ferula asafoetida. Elsevier; 2023. doi: https://doi.org/10.1016/b978-0-323-90794-1.00020-x
- Sood R. Asafoetida (Ferula asafoetida): A high-value crop suitable for the cold desert of Himachal Pradesh, India. Jans. 2020;12(4):607-617. doi: https://doi.org/10.31018/jans.v12i4.2418
- Farhadi F, Asili J, Iranshahy M, Iranshahi M. NMR-based metabolomic study of asafoetida. Fitoterapia. 2019;139:104361. doi: https://doi.org/10.1016/j.fitote.2019.104361
- Ravindran, P.N. Asafoetida | Springer Nature Link [Internet]. 2024 [cited 2026 May 15]. Available from: https://link.springer.com/rwe/10.1007/978-981-19-3728-6_41
- Amalraj A, Gopi S. Biological activities and medicinal properties of Asafoetida: A review. Journal of Traditional and Complementary Medicine. 2017;7(3):347-359. doi: https://doi.org/10.1016/j.jtcme.2016.11.004
- Fierascu RC, Georgiev MI, Fierascu I, Ungureanu C, Avramescu SM, Ortan A, et al. Mitodepressive, antioxidant, antifungal and anti-inflammatory effects of wild-growing Romanian native Arctium lappa L. (Asteraceae) and Veronica persica Poiret (Plantaginaceae). Food and Chemical Toxicology. 2018;111:44-52. doi: https://doi.org/10.1016/j.fct.2017.11.008
- Niazmand R, Razavizadeh BM. Ferula asafoetida: chemical composition, thermal behavior, antioxidant and antimicrobial activities of leaf and gum hydroalcoholic extracts. J Food Sci Technol. 2020;58(6):2148-2159. doi: https://doi.org/10.1007/s13197-020-04724-8
- Alqasoumi S. Anxiolytic effect of Ferula assafoetida L. in rodents. J. Pharmacognosy Phytother. 2012;4(6):86-90. doi: https://doi.org/10.5897/jpp12.027
- Kumar TB, Reddy DVJ, Rushendran R, Mamatha T, Roja J, Roopavani T. Antidepressant activity of ethanolic extract of oleo gum resins of Ferula asafoetida Linn. J Pre Clin Clin Res. 2017;11(1):50-60. doi: https://doi.org/10.26444/jpccr/75721
- Hourfane S, Mechqoq H, Bekkali AY, Rocha JM, El Aouad N. A Comprehensive Review on Cannabis sativa Ethnobotany, Phytochemistry, Molecular Docking and Biological Activities. Plants. 2023;12(6):1245. doi: https://doi.org/10.3390/plants12061245
- Malabadi RB, Kolkar KP, Chalannavar RK, L L, Abdi G. Medical Cannabis sativa (Marijuana or drug type): Psychoactive molecule, Δ9-Tetrahydrocannabinol (Δ9-THC). Ijrias. 2023;VIII(IV):236-249. doi: https://doi.org/10.51584/ijrias.2023.8428
- Wright M, Di Ciano P, Brands B. Use of Cannabidiol for the Treatment of Anxiety: A Short Synthesis of Pre-Clinical and Clinical Evidence. Cannabis & Cannabinoid Research. 2020;5(3):191-196. doi: https://doi.org/10.1089/can.2019.0052
- McPartland JM, Hegman W, Long T. Cannabis in Asia: its center of origin and early cultivation, based on a synthesis of subfossil pollen and archaeobotanical studies. Veget Hist Archaeobot. 2019;28(6):691-702. doi: https://doi.org/10.1007/s00334-019-00731-8
- Schilling S, Melzer R, McCabe PF. Cannabis sativa. Current Biology. 2020;30(1):R8-R9. doi: https://doi.org/10.1016/j.cub.2019.10.039
- Shi ZY, Zeng JZ, Wong AST. Chemical Structures and Pharmacological Profiles of Ginseng Saponins. Molecules. 2019;24(13):2443. doi: https://doi.org/10.3390/molecules24132443
- Wang H, Xu F, Wang X, Kwon WS, Yang DC. Molecular discrimination of Panax ginseng cultivar K-1 using pathogenesis-related protein 5 gene. Journal of Ginseng Research. 2019;43(3):482-487. doi: https://doi.org/10.1016/j.jgr.2018.07.001
- Zhang H, Abid S, Ahn JC, Mathiyalagan R, Kim YJ, Yang DC, et al. Characteristics of Panax ginseng Cultivars in Korea and China. Molecules. 2020;25(11):2635. doi: https://doi.org/10.3390/molecules25112635
- Ginseng | Description, Traditional Medicine, & Species | Britannica [Internet]. 2025 [cited 2025 Jan 30]. Available from: https://www.britannica.com/plant/ginseng
- Hou W, Wang Y, Zheng P, Cui R. Effects of Ginseng on Neurological Disorders. Front. Cell. Neurosci. 2020;14. doi: https://doi.org/10.3389/fncel.2020.00055
- de Oliveira Zanuso B, de Oliveira dos Santos AR, Miola VFB, Guissoni Campos LM, Spilla CSG, Barbalho SM. Panax ginseng and aging related disorders: A systematic review. Experimental Gerontology. 2022;161:111731. doi: https://doi.org/10.1016/j.exger.2022.111731
- Hong UVT, Tamiru-Oli M, Hurgobin B, Okey CR, Abreu AR, Lewsey MG. Insights into opium poppy (Papaver spp.) genetic diversity from genotyping-by-sequencing analysis. Sci Rep. 2022;12(1). doi: https://doi.org/10.1038/s41598-021-04056-3
- Britannica. Opium poppy | Description, Drugs, & Seeds | Britannica [Internet]. 2025 [cited 2025 Jan 31]. Available from: https://www.britannica.com/plant/opium-poppy
- Vadhel A, Bashir S, Mir AH, Girdhar M, Kumar D, Kumar A, et al. Opium alkaloids, biosynthesis, pharmacology and association with cancer occurrence. Open Biol. 2023;13(5). doi: https://doi.org/10.1098/rsob.220355
- Grover P, Bhardwaj M, Mehta L, Chawla PA, Chawla V, Sharma S. Plants with antidengue properties: A systematic review. Elsevier; 2023. doi: https://doi.org/10.1016/b978-0-323-91942-5.00022-7
- Ma L, Ahmeda A, Wang K, Jalalvand AR, Sadrjavadi K, Nowrozi M, et al. Introducing a novel chemotherapeutic drug formulated by iron nanoparticles for the clinical trial studies. Applied Organom Chemis. 2020;36(12). doi: https://doi.org/10.1002/aoc.5498
- Tao W, Dong Y, Su Q, Wang H, Chen Y, Xue W, et al. Liquiritigenin reverses depression-like behavior in unpredictable chronic mild stress-induced mice by regulating PI3K/Akt/mTOR mediated BDNF/TrkB pathway. Behavioural Brain Research. 2016;308:177-186. doi: https://doi.org/10.1016/j.bbr.2016.04.039
- Wang R, Chen Y, Wang Z, Cao B, Du J, Deng T, et al. Antidepressant effect of licorice total flavonoids and liquiritin: A review. Heliyon. 2023;9(11):e22251. doi: https://doi.org/10.1016/j.heliyon.2023.e22251
- Hasan MK, Ara I, Mondal MSA, Kabir Y. Phytochemistry, pharmacological activity, and potential health benefits of Glycyrrhiza glabra. Heliyon. 2021;7(6):e07240. doi: https://doi.org/10.1016/j.heliyon.2021.e07240
- Kenda M, Kočevar Glavač N, Nagy M, Sollner Dolenc M. Medicinal Plants Used for Anxiety, Depression, or Stress Treatment: An Update. Molecules. 2022;27(18):6021. doi: https://doi.org/10.3390/molecules27186021
- Young J, Oakley WR, Fox G. Humulus lupulus and microbes: Exploring biotic causes for hop creep. Food Microbiology. 2023;114:104298. doi: https://doi.org/10.1016/j.fm.2023.104298
- Zanoli P, Rivasi M, Zavatti M, Brusiani F, Baraldi M. New insight in the neuropharmacological activity of Humulus lupulus L. Journal of Ethnopharmacology. 2005;102(1):102-106. doi: https://doi.org/10.1016/j.jep.2005.05.040
- Abdel-Massih RM, El Beyrouthy M. Plants used in Lebanon and the Middle East as Antimicrobials. Elsevier; 2022. doi: https://doi.org/10.1016/b978-0-323-90999-0.00012-4
- Franco L, Sánchez C, Bravo R, Rodriguez A, Barriga C, Juánez J. The sedative effects of hops(Humulus lupulus), a component of beer, on the activity/rest rhythm. Acta Physiologica Hungarica. 2012;99(2):133-139. doi: https://doi.org/10.1556/aphysiol.99.2012.2.6
- Zanoli P, Zavatti M. Neuropharmacological Activity of Humulus Lupulus L. Elsevier; 2009. doi: https://doi.org/10.1016/b978-0-12-373891-2.00054-7
- Corkery JM. Ibogaine as a treatment for substance misuse: Potential benefits and practical dangers. Elsevier; 2018. doi: https://doi.org/10.1016/bs.pbr.2018.08.005
- Launay A. Pharmacognosie, phytochimie, plantes médicinales — cinquième édition J. Bruneton, Éditions Lavoisier Tec & Doc, 2016, 1 488 p, 195,00 €. Phytothérapie. 2017;15(5):316-316. doi: https://doi.org/10.1007/s10298-017-1173-5
- Jenks C. Extraction Studies ofTabernanthe IbogaandVoacanga Africana. Natural Product Letters. 2002;16(1):71-76. doi: https://doi.org/10.1080/1057563029001/4881
- Zubaran C. Noribogaine Generalization to the Ibogaine Stimulus Correlation with Noribogaine Concentration in Rat Brain. Neuropsychopharmacology. 1999;21(1):119-126. doi: https://doi.org/10.1016/s0893-133x(99)00003-2
- Glick SD, Maisonneuve IM, Szumlinski KK. Chapter 2 Mechanisms of action of ibogaine: Relevance to putative therapeutic effects and development of a safer iboga alkaloid congener. Elsevier; 2001. doi: https://doi.org/10.1016/s0099-9598(01)56006-x
- Litjens RPW, Brunt TM. How toxic is ibogaine?. Clinical Toxicology. 2016;54(4):297-302. doi: https://doi.org/10.3109/15563650.2016.1138226
- Sayin HU. Psychoactive Plants Used during Religious Rituals. Elsevier; 2016. doi: https://doi.org/10.1016/b978-0-12-800634-4.00002-0
- Bradshaw AJ, Backman TA, Ramírez-Cruz V, Forrister DL, Winter JM, Guzmán-Dávalos L, et al. DNA Authentication and Chemical Analysis of Psilocybe Mushrooms Reveal Widespread Misdeterminations in Fungaria and Inconsistencies in Metabolites. Appl Environ Microbiol. 2022;88(24). doi: https://doi.org/10.1128/aem.01498-22
- Carod-Artal F. Hallucinogenic drugs in pre-Columbian Mesoamerican cultures. Neurología (English Edition). 2015;30(1):42-49. doi: https://doi.org/10.1016/j.nrleng.2011.07.010
- Lowe H, Toyang N, Steele B, Valentine H, Grant J, Ali A, et al. The Therapeutic Potential of Psilocybin. Molecules. 2021;26(10):2948. doi: https://doi.org/10.3390/molecules26102948
- Arbo MD, Bulcão RP, Rossato LG, Callegari E, Cendron LH, Cabrera ER, et al. Drugs of Abuse and the Internet. Elsevier; 2016. doi: https://doi.org/10.1016/b978-0-12-800213-1.00005-5
- Fricke J, Sherwood AM, Halberstadt AL, Kargbo RB, Hoffmeister D. Chemoenzymatic Synthesis of 5-Methylpsilocybin: A Tryptamine with Potential Psychedelic Activity. J. Nat. Prod. 2021;84(4):1403-1408. doi: https://doi.org/10.1021/acs.jnatprod.1c00087
- Lowe H, Toyang N, Steele B, Valentine H, Grant J, Ali A, et al. The Therapeutic Potential of Psilocybin. Molecules. 2021;26(10):2948. doi: https://doi.org/10.3390/molecules26102948
- Stebelska K. Assays for Detection of Fungal Hallucinogens Such as Psilocybin and Psilocin. Elsevier; 2016. doi: https://doi.org/10.1016/b978-0-12-800212-4.00084-4
- Harari R, Chatterjee I, Getselter D, Elliott E. Psilocybin induces acute anxiety and changes in amygdalar phosphopeptides independently from the 5-HT2A receptor. iScience. 2024;27(5):109686. doi: https://doi.org/10.1016/j.isci.2024.109686
- Santos BWL, Moreira DC, Borges TKDS, Caldas ED. Components of Banisteriopsis caapi, a Plant Used in the Preparation of the Psychoactive Ayahuasca, Induce Anti-Inflammatory Effects in Microglial Cells. Molecules. 2022;27(8):2500. doi: https://doi.org/10.3390/molecules27082500
- Morales-García JA, de la Fuente Revenga M, Alonso-Gil S, Rodríguez-Franco MI, Feilding A, Perez-Castillo A, et al. The alkaloids of Banisteriopsis caapi, the plant source of the Amazonian hallucinogen Ayahuasca, stimulate adult neurogenesis in vitro. Sci Rep. 2017;7(1). doi: https://doi.org/10.1038/s41598-017-05407-9
- White E, Kennedy T, Ruffell S, Perkins D, Sarris J. Ayahuasca and Dimethyltryptamine Adverse Events and Toxicity Analysis: A Systematic Thematic Review. Int J Toxicol. 2024;43(3):327-339. doi: https://doi.org/10.1177/10915818241230916
- Domínguez-Clavé E, Soler J, Elices M, Pascual JC, Álvarez E, de la Fuente Revenga M, et al. Ayahuasca: Pharmacology, neuroscience and therapeutic potential. Brain Research Bulletin. 2016;126:89-101. doi: https://doi.org/10.1016/j.brainresbull.2016.03.002
- National Tropical Botanical Garden [Internet]. [cited 2025 Jul 25]. National Tropical Botanical Garden | Psychotria viridis - Plant Detail - Tropical Plants Database. Available from: https://ntbg.org/
- Daldegan-Bueno D, Simionato NM, Favaro VM, Maia LO. The current state of ayahuasca research in animal models: A systematic review. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2023;125:110738. doi: https://doi.org/10.1016/j.pnpbp.2023.110738
- Rodríguez L, López A, Moyna G, Seoane GA, Davyt D, Vázquez Á, et al. New Insights into the Chemical Composition of Ayahuasca. ACS Omega. 2022;7(14):12307-12317. doi: https://doi.org/10.1021/acsomega.2c00795
- Rossi GN, Guerra LTL, Baker GB, Dursun SM, Saiz JCB, Hallak JEC, et al. Molecular Pathways of the Therapeutic Effects of Ayahuasca, a Botanical Psychedelic and Potential Rapid-Acting Antidepressant. Biomolecules. 2022;12(11):1618. doi: https://doi.org/10.3390/biom12111618
- Soares DB, Duarte LP, Cavalcanti AD, Silva FC, Braga AD, Lopes MT, et al. Psychotria viridis: Chemical constituents from leaves and biological properties. An. Acad. Bras. Ciênc. 2017;89(2):927-938. doi: https://doi.org/10.1590/0001-3765201720160411
- El Euch SK, Hassine D, Cazaux S, Bouzouita N, Bouajila J. Salvia officinalis essential oil: Chemical analysis and evaluation of anti-enzymatic and antioxidant bioactivities. South African Journal of Botany. 2019;120:253-260. doi: https://doi.org/10.1016/j.sajb.2018.07.010
- Ghorbani A, Esmaeilizadeh M. Pharmacological properties of Salvia officinalis and its components. Journal of Traditional and Complementary Medicine. 2017;7(4):433-440. doi: https://doi.org/10.1016/j.jtcme.2016.12.014
- Britannica. Sage | Description, Plant, Herb, Uses, & Facts | Britannica [Internet]. 2024 [cited 2025 Jan 31]. Available from: https://www.britannica.com/plant/sage-plant
- El Gabbas Z, Bezza K, Laadraoui J, Makbal R, Aboufatima R, Chait A. Salvia officinalis induces antidepressant-like effect, anxiolytic activity and learning improvement in hippocampal lesioned and intact adult rats. Bangladesh J Pharmacol. 2018;13(4):367-378. doi: https://doi.org/10.3329/bjp.v13i4.38375
- Xiang T, Wu L, Isah MB, Chen C, Zhang X. Apocynum venetum, a medicinal, economical and ecological plant: a review update. PeerJ. 2023;11:e14966. doi: https://doi.org/10.7717/peerj.14966
- Singh Saroya A, Singh J. Introduction to Psychoactive Medicinal Plants. Singapore: Springer Singapore; 2020. doi: https://doi.org/10.1007/978-981-15-2313-7_1
- Xie W, Zhang X, Wang T, Hu J. Botany, traditional uses, phytochemistry and pharmacology of Apocynum venetum L. (Luobuma): A review. Journal of Ethnopharmacology. 2012;141(1):1-8. doi: https://doi.org/10.1016/j.jep.2012.02.003
- Li X, Wu T, Yu Z, Li T, Zhang J, Zhang Z, et al. Apocynum venetum leaf extract reverses depressive-like behaviors in chronically stressed rats by inhibiting oxidative stress and apoptosis. Biomedicine & Pharmacotherapy. 2018;100:394-406. doi: https://doi.org/10.1016/j.biopha.2018.01.137
- Peterson B, Nguyen H. St. John’s Wort. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 Mar 6]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK557465/ PubMed PMID: 32491397.
- Greeson JM, Sanford B, Monti DA. St. John's wort (Hypericum perforatum): a review of the current pharmacological, toxicological, and clinical literature. Psychopharmacology. 2001;153(4):402-414. doi: https://doi.org/10.1007/s002130000625
- Greeson JM, Sanford B, Monti DA. St. John's wort (Hypericum perforatum): a review of the current pharmacological, toxicological, and clinical literature. Psychopharmacology. 2001;153(4):402-414. doi: https://doi.org/10.1007/s002130000625
- Nobakht SZ, Akaberi M, Mohammadpour AH, Tafazoli Moghadam A, Emami SA. Hypericum perforatum: Traditional uses, clinical trials, and drug interactions. Iran J Basic Med Sci. 2022 Sep;25(9):1045–58. doi:10.22038/IJBMS.2022.65112.14338 PubMed PMID: 36246064; PubMed Central PMCID: PMC9526892.
- Khan H, Nabavi SM. Passiflora (Passiflora incarnata). Elsevier; 2019. doi: https://doi.org/10.1016/b978-0-12-812491-8.00049-7
- USWildflowers.com [Internet]. [cited 2025 Jul 25]. US Wildflower - Purple Passionflower, Maypop - Passiflora incarnata. Available from: https://uswildflowers.com/detail.php?SName=Passiflora%20incarnata
- Janda K, Wojtkowska K, Jakubczyk K, Antoniewicz J, Skonieczna-Żydecka K. Passiflora incarnata in Neuropsychiatric Disorders—A Systematic Review. Nutrients. 2020;12(12):3894. doi: https://doi.org/10.3390/nu12123894
- Passionflower. In: LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012 [cited 2025 Jun 17]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK548020/ PubMed PMID: 31643352.
- Michael HSR, Mohammed NB, Ponnusamy S, Edward Gnanaraj W. A Folk Medicine: <i>Passiflora incarnata</i> L. Phytochemical Profile with Antioxidant Potency. tjps. 2022;19(3):287-292. doi: https://doi.org/10.4274/tjps.galenos.2021.88886
- Viera W, Shinohara T, Samaniego I, Sanada A, Terada N, Ron L, et al. Phytochemical Composition and Antioxidant Activity of Passiflora spp. Germplasm Grown in Ecuador. Plants. 2022;11(3):328. doi: https://doi.org/10.3390/plants11030328
- Golsorkhi H, Qorbani M, Sabbaghzadegan S, Dadmehr M. Herbal medicines in the treatment of children and adolescents with attention-deficit/hyperactivity disorder (ADHD): An updated systematic review of clinical trials. Avicenna J Phytomedicine. 2023;13(4):338–53. doi:10.22038/AJP.2022.21115 PubMed PMID: 37663386; PubMed Central PMCID: PMC10474921.
- Chandrika U, Karunarathna U. Anesthetics and analgesic activities of herbal medicine: Review of the possible mechanism of action. Elsevier; 2022. doi: https://doi.org/10.1016/b978-0-12-818988-7.00003-0
- Fonseca LRD, Rodrigues RDA, Ramos ADS, da Cruz JD, Ferreira JLP, Silva JRDA, et al. Herbal Medicinal Products fromPassiflorafor Anxiety: An Unexploited Potential. The Scientific World Journal. 2020;2020:1-18. doi: https://doi.org/10.1155/2020/6598434
- Salve J, Pate S, Debnath K, Langade D. Adaptogenic and Anxiolytic Effects of Ashwagandha Root Extract in Healthy Adults: A Double-blind, Randomized, Placebo-controlled Clinical Study. Cureus. 2019. doi: https://doi.org/10.7759/cureus.6466
- NCCIH [Internet]. [cited 2025 Jul 25]. Ashwagandha: Usefulness and Safety. Available from: https://www.nccih.nih.gov/health/ashwagandha
- Ashwagandha - Grow To Eat. The Gardener [Internet]. [cited 2025 Jul 25]. Available from: https://www.thegardener.co.za/grow-to-eat/grow-to-eat/ashwagandha/
- Ruhila A, Galib. Ashwagandha (Withania somnifera (Linn.) Dunal). Boca Raton: CRC Press; 2025. doi: https://doi.org/10.1201/9781032675961-35
- Singh N, Bhalla M, De Jager P, Gilca M. An Overview on Ashwagandha: A Rasayana (Rejuvenator) of Ayurveda. Afr. J. Trad. Compl. Alt. Med. 2011;8(5S). doi: https://doi.org/10.4314/ajtcam.v8i5s.9
- Healthline [Internet]. 2021 [cited 2025 Jul 25]. Camellia sinensis Leaf Extract: Benefits, Uses, and Side Effects. Available from: https://www.healthline.com/nutrition/camellia-sinensis-leaf-extract
- Dietz C, Dekker M. Effect of Green Tea Phytochemicals on Mood and Cognition. Cpd. 2017;23(19):2876-2905. doi: https://doi.org/10.2174/1381612823666170105151800
- Sánchez M, González-Burgos E, Iglesias I, Lozano R, Gómez-Serranillos MP. The Pharmacological Activity of Camellia sinensis (L.) Kuntze on Metabolic and Endocrine Disorders: A Systematic Review. Biomolecules. 2020;10(4):603. doi: https://doi.org/10.3390/biom10040603
- Ma GP, Zheng Q, Xu MB, Zhou XL, Lu L, Li ZX, et al. Rhodiola rosea L. Improves Learning and Memory Function: Preclinical Evidence and Possible Mechanisms. Front. Pharmacol. 2018;9. doi: https://doi.org/10.3389/fphar.2018.01415
- Bernatoniene J, Jakstas V, Kopustinskiene DM. Phenolic Compounds of Rhodiola rosea L. as the Potential Alternative Therapy in the Treatment of Chronic Diseases. Ijms. 2023;24(15):12293. doi: https://doi.org/10.3390/ijms241512293
- Panossian A, Wikman G, Sarris J. Rosenroot (Rhodiola rosea): Traditional use, chemical composition, pharmacology and clinical efficacy. Phytomedicine. 2010;17(7):481-493. doi: https://doi.org/10.1016/j.phymed.2010.02.002
- Farooqui AA. Potential Treatment Strategies of Dementia With Ayurvedic Medicines. Elsevier; 2019. doi: https://doi.org/10.1016/b978-0-12-816347-4.00009-x
- Ivanova Stojcheva E, Quintela JC. The Effectiveness of Rhodiola rosea L. Preparations in Alleviating Various Aspects of Life-Stress Symptoms and Stress-Induced Conditions—Encouraging Clinical Evidence. Molecules. 2022;27(12):3902. doi: https://doi.org/10.3390/molecules27123902
- Tao H, Wu X, Cao J, Peng Y, Wang A, Pei J, et al. Rhodiola species: A comprehensive review of traditional use, phytochemistry, pharmacology, toxicity, and clinical study. Medicinal Research Reviews. 2019;39(5):1779-1850. doi: https://doi.org/10.1002/med.21564
- Kennedy DO, Bonnländer B, Lang SC, Pischel I, Forster J, Khan J, et al. Acute and Chronic Effects of Green Oat (Avena sativa) Extract on Cognitive Function and Mood during a Laboratory Stressor in Healthy Adults: A Randomised, Double-Blind, Placebo-Controlled Study in Healthy Humans. Nutrients. 2020;12(6):1598. doi: https://doi.org/10.3390/nu12061598
- Oats | Definition, Types, Nutrition, Uses, & Facts | Britannica [Internet]. [cited 2026 May 16]. Available from: https://www.britannica.com/topic/oats
- Martinez-Horta S, Ivanir E, Perrinjaquet-Moccetti T, Keuter MH, Kulisevsky J. Effects of a Green Oat Herb Extract on Cognitive Performance and Neurophysiological Activity: A Randomized Double-Blind Placebo-Controlled Study. Front. Neurosci. 2021;15. doi: https://doi.org/10.3389/fnins.2021.748188
- Bocquet L, Sahpaz S, Hilbert JL, Rambaud C, Rivière C. Humulus lupulus L., a very popular beer ingredient and medicinal plant: overview of its phytochemistry, its bioactivity, and its biotechnology. Phytochem Rev. 2018;17(5):1047-1090. doi: https://doi.org/10.1007/s11101-018-9584-y
- Kwakye GF, Jiménez J, Jiménez JA, Aschner M. Atropa belladonna neurotoxicity: Implications to neurological disorders. Food and Chemical Toxicology. 2018;116:346-353. doi: https://doi.org/10.1016/j.fct.2018.04.022
- Gibbons S. Plants as a Source of Bacterial Resistance Modulators and Anti-Infective Agents. Phytochem Rev. 2005;4(1):63-78. doi: https://doi.org/10.1007/s11101-005-2494-9
- Fasinu PS, Bouic PJ, Rosenkranz B. An Overview of the Evidence and Mechanisms of Herb–Drug Interactions. Front. Pharmacol. 2012;3. doi: https://doi.org/10.3389/fphar.2012.00069
- Heinrich M, Mah J, Amirkia V. Alkaloids Used as Medicines: Structural Phytochemistry Meets Biodiversity—An Update and Forward Look. Molecules. 2021;26(7):1836. doi: https://doi.org/10.3390/molecules26071836
- Izzo AA, Ernst E. Interactions Between Herbal Medicines and Prescribed Drugs. Drugs. 2009;69(13):1777-1798. doi: https://doi.org/10.2165/11317010-000000000-00000
- Sarris J, McIntyre E, Camfield DA. Plant-Based Medicines for Anxiety Disorders, Part 1. CNS Drugs. 2013;27(3):207-219. doi: https://doi.org/10.1007/s40263-013-0044-3
- Johnson MW, Griffiths RR, Hendricks PS, Henningfield JE. The abuse potential of medical psilocybin according to the 8 factors of the Controlled Substances Act. Neuropharmacology. 2018;142:143-166. doi: https://doi.org/10.1016/j.neuropharm.2018.05.012
- Ahmad Khan MS, Ahmad I. Herbal Medicine. Elsevier; 2019. doi: https://doi.org/10.1016/b978-0-12-814619-4.00001-x
- Sayin U. A Comparative Review of the Neuro-Psychopharmacology of Hallucinogen-Induced Altered States of Consciousness: The Uniqueness of Some Hallucinogens. Neuroquantology. 2012;10(2). doi: https://doi.org/10.14704/nq.2012.10.2.528
- Sayin U. Altered States of Consciousness Occurring During Expanded Sexual Response In The Human Female: Preliminary Definitions. Neuroquantology. 2011;9(4). doi: https://doi.org/10.14704/nq.2011.9.4.486
- Sayin HU. The Consumption of Psychoactive Plants in Ancient Global and Anatolian Cultures During Religious Rituals: The Roots of the Eruption of Mythological Figures and Common Symbols in Religions and Myths. Neuroquantology. 2014;12(2). doi: https://doi.org/10.14704/nq.2014.12.2.753