RESEARCH ARTICLE
Vaccine Decision-Making in Kaliombo Village: The Role of Halal Awareness, Emergencies, and Religiosity
Halal Science|Vol. 1, Issue 2, pp. 31-36 (2025)
CC BY 4.0-2025 Authors
Views
Downloads
Shares
Received
Sep 27, 2025Revised
Nov 10, 2025Accepted
Nov 19, 2025Published
Nov 28, 2025
Abstract
The controversy surrounding the halal status of the AstraZeneca COVID-19 vaccine, combined with the urgency of pandemic control efforts, has raised concerns among Muslim communities, particularly in rural settings. This study examines the effects of halal awareness, perceived emergency conditions, and religiosity on individuals’ decisions to receive the AstraZeneca vaccine in Kaliombo Village, Bojonegoro Regency. A quantitative survey involving 112 respondents was analyzed using multiple regression, t-tests, F-tests, and Moderated Regression Analysis (MRA). The results show that halal awareness has a statistically significant direct effect on vaccination decisions (t = 2.227, p = 0.028), whereas perceived emergency conditions do not (t = 1.803, p = 0.074). Together, halal awareness and emergency conditions significantly influence vaccination decisions (F = 9.253, p < 0.001), though their explanatory power remains modest (R² = 0.145). Religiosity does not moderate these relationships but functions as an independent predictor (t = 2.653, p = 0.009), increasing the explained variance to 17.5% (R² = 0.175). While statistically significant, these effects are substantively modest, indicating that behavioral decisions are shaped by multiple social and contextual factors. Overall, the findings highlight the prominent role of halal awareness and religiosity in vaccine acceptance and underscore the need to integrate religious considerations into public health communication strategies.
Introduction
The rapid global spread of Coronavirus Disease 2019 (COVID-19) has posed major challenges to public health systems, with more than 6 million confirmed cases and significant mortality reported in Indonesia (1, 2). Vaccination is recognized as one of the most effective strategies to curb transmission and reduce disease severity (3, 4). However, vaccine uptake remains uneven, with national surveys indicating that more than 30% of Indonesians expressed hesitancy toward COVID-19 vaccination (5). Among the main reasons for refusal were concerns about safety, perceived ineffectiveness, and, importantly, doubts regarding the halal status of vaccines such as AstraZeneca, which reportedly involve porcine-derived materials in their production (6, 7)
This issue highlights a critical dilemma in Indonesia, where the majority of the population is Muslim and religious principles strongly influence health-related decisions. The urgency of mass vaccination during a declared public health emergency has necessitated religious deliberation (8, 9). In 2021, the Indonesian Ulema Council (MUI) issued a fatwa declaring the AstraZeneca vaccine haram due to the use of porcine trypsin, yet permissible under emergency conditions (10, 11). While this ruling was intended to reduce public resistance, challenges remain in aligning halal awareness, perceptions of emergency, and individual religiosity with collective health needs (12). These factors interact to shape vaccination decisions, creating a complex socio-religious context for pandemic response.
Previous studies on halal awareness and religiosity largely focus on consumer behavior in food and cosmetics, with limited exploration in public health interventions such as vaccination (13, 14). Moreover, while some research acknowledges the moderating role of religiosity, findings remain inconsistent, pointing to the need for further empirical testing (15). This study addresses that gap by examining the influence of halal awareness and perceived COVID-19 emergency on the decision to use the AstraZeneca vaccine, with religiosity as a moderating variable, in Kaliombo Village, Purwosari District, Bojonegoro. Kaliombo Village was selected due to documented lower vaccination coverage in the Purwosari District compared to surrounding areas, and because local health office reports identify halal concerns as a primary reason for AstraZeneca refusal in this village, which has a highly religious community profile.
Using a quantitative survey with regression and moderation analysis, this research provides new insights into the intersection of religion, health, and decision-making (16). The study specifically aims to assess whether halal awareness and perceived emergency significantly influence vaccine-use decisions, and whether religiosity alters the strength of these relationships within a community where religious norms strongly guide behavioral choices. The findings are expected to inform both policy and community-level strategies for strengthening public trust and compliance in vaccination programs during health crises.
Methodology
Study Design and Setting
This study employed a quantitative, cross-sectional research design to examine the influence of halal awareness and the COVID-19 emergency context on the decision to receive the AstraZeneca COVID-19 vaccine, with religiosity as a moderating variable. The study was conducted in Kaliombo Village, Purwosari District, Bojonegoro Regency, Indonesia, a predominantly Muslim rural community that provides a relevant context for examining religiously influenced health decisions.
Research Setting and Study Area
The research took place in Kaliombo Village, Purwosari District, Bojonegoro Regency, East Java, Indonesia. Kaliombo is a rural area with a predominantly Muslim population, where religious values strongly guide daily practices, including health-related decisions. During the COVID-19 pandemic, the village was targeted by the government’s mass vaccination program, yet community acceptance of the AstraZeneca vaccine was undermined by concerns about its halal status due to reports of porcine-derived components in production. The selection of Kaliombo as the study site was deliberate, as it reflects the socio-religious dynamics of Muslim-majority rural communities and illustrates the practical challenges of implementing vaccination campaigns in settings where religious considerations strongly influence public health behaviors.
Population, Sample, and Sampling
The target population consisted of adult residents of Kaliombo Village who were eligible for COVID-19 vaccination. Based on population records, 155 residents were identified as the accessible population. Using simple random sampling, 112 respondents were selected as the final sample, a size considered sufficient to achieve statistical power for multiple regression analysis. Inclusion criteria required participants to be (i) at least 18 years old, (ii) residents of the study site, and (iii) eligible for COVID-19 vaccination. Individuals unwilling to provide informed consent were excluded.
Instruments and Variables
Data were collected using a structured questionnaire developed from validated instruments in prior studies and adapted to the vaccination context. The questionnaire measured four main constructs: (i) halal awareness, (ii) perception of COVID-19 emergency, (iii) religiosity, and (iv) vaccination decision-making. Each construct was operationalized through multiple items rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Independent variables included halal awareness and perception of emergency; religiosity functioned as a moderating variable; and the decision to vaccinate with AstraZeneca served as the dependent variable.
Procedures Respondents were approached directly and participated after providing informed consent. The questionnaire was self-administered, with researchers available for clarification when needed. To ensure reliability and validity, the instrument underwent pre-testing with 20 respondents from a comparable population. Reliability was assessed using Cronbach’s alpha, with values above 0.70 deemed acceptable. Content validity was established through expert review by three specialists in Islamic economics and public health.
Data Analysis
Data were analyzed using t-tests, F-tests, multiple linear regression, and moderated regression analysis (MRA). Prior to hypothesis testing, datasets were evaluated for completeness, normality, multicollinearity, and heteroscedasticity. All continuous predictor variables were mean-centered before constructing interaction terms to reduce multicollinearity and meet MRA assumptions. Statistical significance was set at p < 0.05, and coefficients of determination (R²) were reported to assess explanatory power.
Results
Respondents’ Demographic Characteristics
Respondents were required to meet three inclusion criteria: (i) residents of Kaliombo Village, Purwosari District, Bojonegoro Regency; (ii) adherents of Islam; and (iii) recipients of the AstraZeneca COVID-19 vaccine. A total of 112 respondents fulfilled these criteria. Table 1 summarizes their demographic characteristics.
| Variable | Category | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Gender | Male | 41 | 36.6 |
| Female | 71 | 63.4 | |
| Age (years) | 21–30 | 20 | 17.9 |
| 31–40 | 44 | 39.3 | |
| 41–50 | 33 | 29.5 | |
| > 50 | 15 | 13.3 | |
| Occupation | Civil servant | 11 | 9.8 |
| Private employee | 38 | 33.9 | |
| Entrepreneur | 30 | 26.8 | |
| Farmer | 25 | 22.3 | |
| Others | 8 | 7.2 | |
| Education | Elementary school | 21 | 18.8 |
| Junior high school | 31 | 27.7 | |
| Senior high school | 47 | 42.0 | |
| Higher education | 13 | 11.6 | |
| Vaccination status | Vaccinated (≥1 dose) | 81 | 72.3 |
| Not vaccinated | 31 | 27.7 |
Instrument Validity and Reliability
All measurement items were subjected to validity testing using item-total correlations with r-table = 0.3494 (α = 0.05). Items exceeding this threshold were retained. Reliability was assessed using Cronbach’s Alpha and demonstrated excellent internal consistency (α = 0.940). The summary is shown in Table 2.
| Variable | Total Items | Valid Items | Invalid Items | Cronbach’s Alpha |
|---|---|---|---|---|
| Halal Awareness (X1) | 19 | 15 | 4 | 0.940 |
| COVID – 19 Emergency | 14 | 12 | 2 | 0.940 |
| Vaccination Decision | 9 | 9 | 0 | 0.940 |
| Religiosity | 14 | 13 | 1 | 0.940 |
Validity Test Results
To ensure regression accuracy, classical assumption tests were performed:
Normality
Kolmogorov–Smirnov testing showed p = 0.474, indicating normally distributed residuals.
Multicollinearity
Tolerance values (> 0.10) and VIF scores (1.462–2.022) demonstrated an absence of multicollinearity. All continuous predictors were mean-centered before creating interaction terms for MRA.
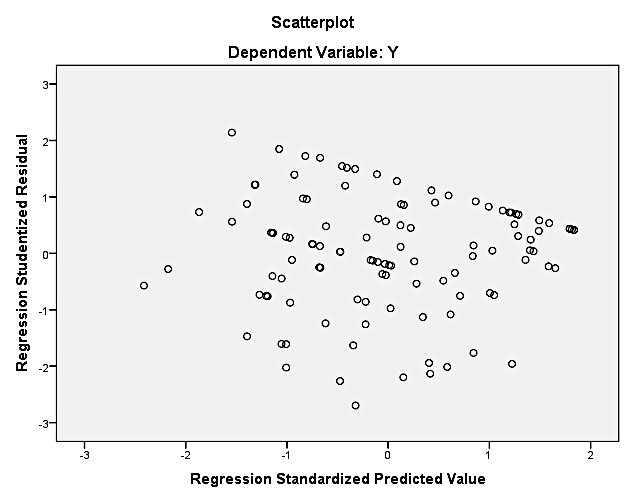
Heteroscedasticity
The heteroscedasticity test was conducted to assess the stability of error variances using a scatterplot of standardized residuals against predicted values (see Figure 1). Heteroscedasticity is indicated when residuals form visible patterns, clusters, or funnel-shaped distributions, whereas the absence of a clear pattern characterized by residuals randomly dispersed above and below the zero line reflects homoscedasticity. Visual inspection of the scatterplot showed that the residuals were spread randomly without forming any systematic or directional pattern, indicating stable error variance and confirming that heteroscedasticity was not present in the data.
Partial Effects (t-Test)
Regression analysis demonstrated that Halal Awareness (X1) had a significant positive effect on Vaccination Decision (t = 2.227, p = 0.028). COVID-19 Emergency Condition (X2) did not significantly affect Vaccination Decision (t = 1.803, p = 0.074). Thus, H1 is supported, whereas H2 is not supported.
Simultaneous Effects (F-test and R²)
The model comprising X1 and X2 was statistically significant (F = 9.253, p < 0.001). The coefficient of determination (R² = 0.145) indicates that both predictors jointly explain 14.5% of the variance in vaccination decision
Multiple Linear Regression Model
The general form of the regression model used can be seen in Eq. 1. The estimated model obtained from the data is described in Eq. 2. Each one-unit increase in Halal Awareness increases the likelihood of choosing the AstraZeneca vaccine by 0.207 units (significant). Each one-unit increase in Emergency Condition increases the decision score by 0.176 units, but the effect is not significant.
Moderated Regression Analysis (MRA)
Moderation analysis was conducted to assess whether religiosity alters the strength of the relationships between both predictors (X₁ and X₂) and vaccination decisions. All continuous variables were mean-centered before generating interaction terms.
Moderation of Halal Awareness
The conceptual moderation model can be seen in Eq. 3. Empirical estimation produced is described in Eq. 4. The interaction term was not significant (p = 0.092), indicating that religiosity does not moderate the effect of Halal Awareness on vaccination decisions.
Y=73.202−0.952X1−0.865M+0.020(X1×M)Y=73.202−0.952X1−0.865M+0.020(X1×M)(Eq. 4)
Moderation of COVID-19 Emergency
The moderation model is represented conceptually as seen in Eq. 5. The estimated model is described in Eq. 6. The interaction effect was again non-significant (p = 0.226), confirming that religiosity does not moderate the relationship between perceived emergency conditions and vaccination decisions. Across both analyses, religiosity consistently acted as an independent predictor, not a moderator.
Y=73.2−0.95X1−0.865M+0.02(X1×M)Y=73.2−0.95X1−0.865M+0.02(X1×M)(Eq. 6)
Final Combined Regression Model
To evaluate the collective influence of all predictors, a full regression model was estimated using Halal Awareness (X₁), COVID-19 Emergency (X₂), and Religiosity (X₃). The general form of the model is shown in Eq. 7. The empirical model derived from the data is described in Eq. 8.
In this combined model, Religiosity (b = 0.238, p = 0.009) emerged as the strongest and only significant predictor of vaccination decisions. Halal Awareness and perceived emergency conditions showed positive but non-significant contributions when analyzed alongside religiosity. The model overall was significant (F = 8.857, p < 0.001), indicating that all three predictors jointly influence vaccination decisions, even though individual significance differs.
Discussion
The statistical analysis demonstrates that halal awareness, religiosity, and the perception of COVID-19 emergency conditions contribute to the community’s decision to receive the AstraZeneca vaccine, although their effects vary in strength and statistical significance. The t-test results indicate that halal awareness has a positive and significant effect on vaccination decision (t = 2.227, p = 0.028 < 0.05). This finding suggests that individuals who are more attentive to halal issues tend to be more receptive toward vaccines they perceive as religiously permissible or sufficiently justified under emergency conditions. These results align with previous studies such as Utami and Genoveva (2020) (17), who found that halal awareness shapes decision-making in other halal-sensitive contexts, though they contrast with findings by Hervina et al. (2021) (18), who reported non-significant effects in digital food purchasing during the pandemic. Such inconsistencies highlight that the influence of halal awareness is highly context-dependent, particularly when the product in question such as a vaccine directly intersects with health, religious rulings, and public trust.
Religiosity also shows a significant positive influence on vaccination decisions (t = 2.653, p = 0.009 < 0.05). This reinforces the idea that religious commitment shapes individual attitudes toward health interventions, especially when these interventions involve halal considerations or rely on religious authorities for legitimacy. Earlier studies, such as Iriani (19), similarly emphasize that religiosity encourages individuals to align behaviors with religious teachings. In the context of COVID-19 vaccination, strong religious values may encourage acceptance once a fatwa or religious guideline permits vaccination under emergency conditions. This indicates that religiosity does not merely complement halal awareness but can become a primary psychological driver in shaping attitudes toward vaccination (20).
In contrast, the perception of COVID-19 emergency conditions does not exhibit a significant partial effect on vaccination decision (t = 1.803, p = 0.074 > 0.05). Although the pandemic created considerable fear, uncertainty, and public health risk, the respondents in this study appeared less influenced by the perceived level of emergency and more influenced by religious legitimacy and personal beliefs. This non-significance is particularly important, as it suggests that during prolonged crises, communities may experience “risk normalization” a condition wherein individuals become less responsive to emergency cues because these conditions become part of everyday life. This phenomenon has been observed in other long-duration health crises, where emotional reactions to risk diminish over time, reducing the weight of perceived emergency in decision-making.
The Moderated Regression Analysis (MRA) further indicates that religiosity does not operate as a moderator in the relationship between halal awareness or emergency conditions and vaccination decisions. Although religiosity demonstrates a significant direct influence (p = 0.007 < 0.05), neither the interaction between religiosity and halal awareness (p = 0.092 > 0.05) nor the interaction between religiosity and emergency conditions (p = 0.226 > 0.05) reaches statistical significance. This pattern suggests that religiosity functions as an independent psychological predictor rather than a factor that strengthens or weakens the effect of the other variables. In other words, religiosity shapes vaccination decisions in parallel with halal considerations, not as a mechanism that modifies their influence.
Simultaneous testing using the F-test confirms that halal awareness, emergency conditions, and religiosity collectively exert a significant influence on vaccination decisions (F = 8.857, p < 0.001). The coefficient of determination (R² = 0.175) indicates that these three variables explain 17.5% of the variance in vaccination decision-making, while the remaining 82.5% is influenced by other factors such as misinformation, family influence, trust in healthcare workers, prior vaccine experiences, and exposure to religious opinions.
Overall, the findings highlight the centrality of halal awareness and religiosity in shaping vaccination acceptance within Muslim-majority communities, while also underscoring the limited role of perceived emergency conditions. From a practical standpoint, this suggests that strengthening public understanding of halal rulings, clarifying religious legitimacy for vaccines, and collaborating closely with religious leaders may be more effective strategies for increasing vaccine uptake than relying solely on emergency risk communication. For policymakers, the results emphasize that halal assurance and religious endorsement should not be viewed merely as symbolic gestures but as essential components of health communication strategies within religious communities.
Conclusion
The findings of this study show that halal awareness significantly influences individuals’ decisions to receive the AstraZeneca COVID-19 vaccine, while perceptions of emergency conditions alone do not. Religiosity does not act as a moderator but emerges as a strong independent predictor that operates alongside halal awareness in shaping vaccination choices, underscoring the prominent role of religious values in vaccine acceptance within Muslim communities. These results indicate that religious considerations weigh more heavily than situational risk perceptions when individuals evaluate the permissibility and safety of vaccination. However, the study is limited by its cross-sectional design, its reliance on self-reported data, and the focus on a single rural village, which may constrain the generalizability and causal interpretation of the findings. Future research should therefore employ multi-site samples, longitudinal designs, and complementary behavioral measures to strengthen empirical robustness.
Building on these findings, several recommendations can be proposed. Public health authorities should strengthen collaboration with religious leaders to communicate halal assurances clearly and consistently, particularly in contexts where vaccine acceptance is influenced by religious rulings. Educational efforts should emphasize both the religious legitimacy and scientific rationale underlying emergency-use fatwas to address lingering doubts among Muslim communities. Tailored health communication strategies that integrate religious perspectives may enhance trust, reduce hesitancy, and improve vaccination uptake in similar socio-religious settings.
Declarations
Conflict of Interest
The authors declare no conflicting interest.
Data Availability
All data generated or analyzed during this study are included in this published article.
Funding Information
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
References
- Novarisa N, Helda, Mulyadi R. Indonesia’s COVID-19 trend after the end of a public health emergency of international concern: preparation for an endemic. Kesmas. 2023 Jul 1;18(1):25–30.
- Rozaliyani A, Savitri AI, Setianingrum F, Shelly TN, Ratnasari V, Kuswindarti R, et al. Factors associated with death in COVID-19 patients in Jakarta, Indonesia: an epidemiological study. Acta Med Indones. 2020;52.
- Li H, Zhu X, Yu R, Qian X, Huang Y, Chen X, et al. The effects of vaccination on the disease severity and factors for viral clearance and hospitalization in Omicron-infected patients: a retrospective observational cohort study from recent regional outbreaks in China. Front Cell Infect Microbiol. 2022 Nov 7;12.
- Lotfi H, Mazar MG, Ei NMH, Fahim M, Yazdi NS. Vaccination is the most effective and best way to avoid the disease of COVID-19. Immun Inflamm Dis. 2023;11.
- Sujarwoto, Maharani A, Holipah, Andarini S, Saputri RAM, Pakpahan E, et al. Understanding COVID-19 vaccine hesitancy: a cross-sectional study in Malang District, Indonesia. Front Public Health. 2023 Jan 26;10.
- Made Ayu Sukma Widyandari N, Wayan Edi Sanjana I. Key point of COVID-19 pandemic management as global disaster in nursing perspective: a scooping review. Jurnal Keperawatan. 2022.
- Harapan BN, Harapan T, Theodora L, Anantama NA. From archipelago to pandemic battleground: unveiling Indonesia’s COVID-19 crisis. J Epidemiol Glob Health. 2023 Sep 14;13(4):591–603.
- Giubilini A, Savulescu J, Wilkinson D. Which vaccine? The cost of religious freedom in vaccination policy. J Bioeth Inq. 2021 Dec 1;18(4):609–19.
- Mahsun M, Khoir T, Mufrikhah S, Masrohatun, Hashim S. The strategic role of religious authority in supporting state policy on non-natural disaster management in Indonesia. Jurnal Theologia. 2024 Jun 25;36(1):51–70.
- Rachmawati A, Hisan K. The review of emergency concept in Islamic law towards the fatwa of the Indonesian Ulema Council No. 14 of 2021 on the use of AstraZeneca’s COVID-19 vaccine. J Indones Comp Syariah Law. 2022;5(2).
- Anisa. Comparative study of the ijtihad method of the Indonesian Ulema Council and Bahtsul Masail Nahdlatul Ulama on the fatwa of the AstraZeneca vaccine. J Islamic Legal Stud. 2021 Jul.
- Awaliah Kasri R, Amalia N, Miranti Yuniar A, Mariz K. Opportunities and challenges for developing halal pharmaceuticals industry in Indonesia. Int J Halal Res. 2023;5.
- Nurrahmi N, Kaban RF, Widjaja HS. The effects of religiosity and halal knowledge on the decision to use the COVID-19 vaccine. Ilomata Int J Soc Sci. 2023 Jul 31;4(3):376–89.
- Sudarsono H, Ikawati R, Azizah SN, Kurnia A, Nuanmark P. Does “halalness” affect young Muslims’ intentions to use the COVID-19 vaccine? Indones J Halal Res. 2023 Feb 1;5(1):30–40.
- Raharja BS, Sari DH. Critical factors affecting the participation in COVID-19 vaccination program in Residency of Surakarta: the extended theory of planned behaviour. J Manaj Teor Terapan. 2022 Aug 27;15(2):196–208.
- Hana Haninda S, Amalia Elfita R. The moderating role of religiosity on ethical behavioral intention: planned behavioral theory approach. Bus Finance J. 2022 Mar.
- Genoveva G, Utami NN. The influence of brand image, halal label, and halal awareness on customers purchasing decision of halal cosmetic. J Muara Ilmu Ekon Bisnis. 2020 Aug 22;4(2):355.
- Dhea Hervina R, Fitriana Kaban R, Novita Pasaribu P. Pengaruh kesadaran halal dan harga terhadap keputusan pembelian konsumen GoFood di era pandemi COVID-19. Inovator J Manaj. 2021;10(2):133–40.
- Iriana SS. The effect of religiosity on the purchasing decisions of halal labeled food products. East Afr Scholars J Econ Bus Manag. 2019;621–8.
- Mahadewi EP, Hidayat Sutawidjaya A, Asih D, Surip N, Harahap A. Sustainable marketing of healthcare in Indonesia with religiosity and health promotion clean healthy lifestyle. BIRCI J. 2022.