
RESEARCH ARTICLE
Effectiveness of TB-Reminder Application in Improving Medication Adherence and Quality of Life of Lung Tuberculosis Patients in Indonesia
Academic Editor: Ahmed Mohsin Mahdi
Sciences of Pharmacy|Vol. 4, Issue 3, pp. 117-126 (2025)
CC BY 4.0-2025 Authors
Views
Downloads
Shares
Received
May 19, 2025Revised
Jun 21, 2025Accepted
Jun 23, 2025Published
Jul 4, 2025
Abstract
Poor adherence to anti-tuberculosis (TB) treatment continues to hinder therapeutic success and patient quality of life. This study aimed to evaluate the effectiveness of the TB-R mobile application in improving medication adherence and quality of life among pulmonary TB patients at Pandeglang Regional Hospital. Eighty-six patients were randomized into intervention (n = 43) and control (n = 43) groups. Adherence and quality of life were measured using the Medication Adherence Rating Scale (MARS) and EQ-5D-5L, respectively. After one month, the intervention group demonstrated significantly higher adherence (97.7% vs. 79.0%, p < 0.001) and improvement in mean MARS scores (24.7 vs. 22.7, p < 0.001). Although quality of life gains were not statistically significant overall, notable improvements were observed in anxiety/depression and self-care domains. Demographic factors influenced outcomes: patients aged 29–39 and those living with others showed better adherence, while patients aged 40–50 experienced greater quality of life gains. Women aged 51–60 living alone had decreased adherence despite quality of life improvements. These results suggest that mHealth tools like TB-R can enhance adherence, especially when supported by favorable social and demographic conditions. Tailored digital interventions may optimize treatment outcomes in TB care. Future mHealth app development should consider these social and demographic factors to maximize effectiveness and user engagement.
Keywords:
Introduction
Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis that primarily affects the lungs and is marked by the formation of granulomas (1). TB remains a major public health concern in Indonesia, with 260,699 bacteriologically confirmed cases reported in 2019, accounting for 97.25 cases per 100,000 population (2). Despite being curable with appropriate therapy, TB requires a long treatment duration, typically consisting of two phases: an intensive phase of two months followed by a continuation phase lasting four to seven months, depending on the patient’s condition (3).
This prolonged therapy often leads to decreased adherence due to factors such as pill burden, drug toxicity, and side effects (4). Yet, adherence to anti-TB medication is critical to prevent disease progression, reduce transmission, and avoid drug resistance (5). Adherence itself is influenced by a range of behavioral, psychological, and socioeconomic factors, making it a complex and dynamic issue (6). Despite the presence of the national TB program under Indonesia’s Ministry of Health, which includes DOTS (Directly Observed Treatment, Short-course) and community-based initiatives, significant gaps remain—especially in remote and underserved regions where health infrastructure, patient supervision, and digital integration are limited (7). These limitations hinder consistent treatment adherence and highlight the need for complementary solutions. The extended course of treatment also impacts patients’ physical and mental health, contributing to a decline in overall quality of life (8, 9). Studies show that poor quality of life among TB patients is linked to incomplete treatment, which can further hinder recovery (10, 11). For instance, Ita et al. (2020) found that TB patients in underserved communities experience a lower quality of life, often due to limited social support, psychological stress, and poor treatment adherence (12). Similarly, Alfauzan and Lucya (2021) reported that TB patients in several Asian countries exhibit suboptimal quality of life, with low adherence cited as a contributing factor (13). Both studies primarily examined traditional interventions involving direct patient counseling and community-based support, rather than digital or mobile-based approaches. These findings highlight the need for targeted interventions to address adherence-related challenges in TB treatment.
The World Health Organization (WHO) emphasizes the potential of digital health interventions to improve access, adherence, and health outcomes (14). Mobile technologies, particularly smartphone applications, are increasingly recognized as effective tools for enhancing treatment engagement. One of the rapidly growing forms of digital intervention is mobile health (mHealth) applications, which offer a personalized, interactive, and real-time approach to supporting chronic disease management including TB (15, 16). Global evidence suggests that mHealth applications are effective in improving treatment adherence in TB patients, particularly through medication reminders, symptom tracking, and health education features (17, 18). Research suggests that digital interventions, such as mHealth apps with reminder systems and interactive content, can enhance engagement and adherence in TB treatment (16). Prior implementations in high TB burden countries, including India, South Africa, and China, have demonstrated that mobile reminders significantly increase medication adherence and follow-up completion (15).
In Indonesia, the high prevalence of smartphone use, especially among younger, productive-age populations, offers a promising platform for digital health delivery. As of 2024, approximately 78% of Indonesia’s population (over 215 million people) are internet users, with mobile devices being the dominant access point (19). Several mobile health initiatives have been piloted in Indonesia in other health areas, demonstrating practical feasibility in similar socio‑demographic settings. For instance, a 2023 qualitative study in Jakarta explored early antenatal care delivery through an mHealth system, showing improved service quality and user acceptance among pregnant women and midwives. Another 2023 survey of the “WANTER” app in rural West Java found significant enhancements in anemia-related knowledge and iron‑folic acid adherence among female students (20). Additionally, an international literature review including Indonesian studies confirmed that Android‑based antenatal care apps effectively increased ANC visits and maternal health engagement (21). Given that TB often affects individuals in younger and working-age groups, digital interventions targeting smartphones, especially Android, the most widely used operating system in Indonesia, are well positioned to improve adherence in this population.
Although adherence to anti-TB therapy remains suboptimal in many regions (7, 15-16), few digital tools have been locally developed to address this issue, particularly in underserved areas like Pandeglang district, Banten province. The Tuberculosis Reminder (TB-R) application is an Android-based app designed to support TB patients through two key features: daily medication reminders and educational content related to TB. These features aim to promote consistent medication intake and enhance patient awareness of their treatment regimen. This study aimed to evaluate the effectiveness of the TB-R mobile application in improving medication adherence and quality of life among pulmonary TB patients at Pandeglang Regional Hospital.
Methodology or Experimental Section
TB-R Application Development
The TB-R (Tuberculosis Reminder) application is built as an integrated mobile-based system, allowing patients to receive medication reminders via smartphones and internet-based devices. The app was hosted using a stable cloud-based server to ensure reliability, uptime, and secure access across different regions. A simple and memorable domain name was used to allow users to easily access the service. In terms of user experience, the TB-R app was designed with a clean, responsive interface optimized for Android devices. It features intuitive navigation and lightweight architecture to ensure smooth performance even on low- to mid-range smartphones. The core functionality includes high-precision daily medication reminders synchronized to patient schedules, and interactive educational modules. These features aim to enhance patient engagement and improve adherence behaviors through consistent digital support. The combination of a responsive application system, stable server, and easily accessible domain makes TB-R a reliable digital solution in supporting the treatment of tuberculosis patients.
Sample and Population
This study was conducted at the Lung Polyclinic of Berkah Pandeglang Regional Hospital, Banten, Indonesia. The target population included adult pulmonary tuberculosis (TB) patients receiving care at the facility. Inclusion criteria were: patients aged 18–65 years, currently undergoing the continuation phase of category I anti-tuberculosis therapy, and willing to participate by providing signed informed consent. Category I therapy includes an initial two-month intensive phase consisting of rifampicin, isoniazid, pyrazinamide, and ethambutol, followed by a four-month continuation phase with rifampicin and isoniazid.
Exclusion criteria included patients who (1) did not complete the pre-intervention (pre-test) assessment, (2) were in the final month of treatment (i.e., nearing completion of therapy), or (3) could not be followed up due to loss of contact or death during the study period. Participants were recruited using purposive sampling, guided by clinic staff's eligibility screening based on medical records and interviews. Randomization was carried out using a computer-generated random number table by a third-party researcher who was not involved in data collection or analysis, ensuring allocation concealment. The minimum required sample size was calculated using Slovin’s formula and can be seen in Eq. 1.
Where n is the sample size, N (133 patient) is the total population of eligible TB patients at the facility, and e is the margin of error (set at 10%). Based on this calculation, a minimum of 63 participants was required. To account for potential attrition or exclusions, 85 patients were initially recruited.
Eligible participants were then randomly allocated into two groups: the intervention group (n = 43), who used the TB-R app, and the control group (n = 43), who received standard care without the use of the TB-R app. Randomization was performed using simple random sampling generated by computer software (Microsoft Excel RAND function) to ensure unbiased allocation and strengthen internal validity. This study received ethical approval from the Health Research Ethics Committee of Respati University of Yogyakarta (No. 110.3/FIKER/PL/VIII/2024, dated August 12, 2024).
Blinding was not feasible for participants due to the nature of the intervention (mobile application use), but outcome assessors and data analysts were blinded to group allocation to reduce assessment bias. Potential confounders such as age, gender, employment status, and education level were measured and included in multivariate models to control for their effects on outcome measures.
Data Collection and Preparation
This study employed a quantitative experimental design using a pretest-posttest control group approach. Data collection was conducted over a one-month period among pulmonary tuberculosis (TB) patients treated at Berkah Pandeglang Regional Hospital.
Participants in the intervention group received access to the TB-R app, which contains educational materials and a medication reminder feature. Educational content was delivered through nine interactive myth-versus-fact modules covering key aspects of pulmonary TB, including its definition, etiology, risk factors, treatment protocols, and transmission prevention. The application also includes a Medicine Alarm feature that provides daily reminders for taking anti-tuberculosis medication, tailored to the patient’s treatment schedule. Participants in the intervention group were trained in-person by a research assistant on how to download, navigate, and use the TB-R app. App usage was monitored weekly via app log records and follow-up calls to encourage compliance.
The TB-R app is freely available for Android users via the Google Play Store. During the intervention period, participants were instructed to use the app consistently throughout their prescribed medication regimen for one month.
Data collection tools included two standardized and validated instruments:
1. Medication Adherence Rating Scale (MARS): to assess adherence behavior in taking anti-tuberculosis drugs. The MARS is a five-item self-report scale, with each item rated on a 5-point Likert scale (1 = always, 5 = never). Total scores range from 5 to 25, with higher scores indicating better adherence. In this study, a score above 20 was considered indicative of high adherence.
2. European Quality of Life-5 Dimensions-5 Levels (EQ-5D-5L): to evaluate patient quality of life across five dimensions. Each of the five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) is rated on five levels from “no problems” to “unable”. These responses are converted into a single index score using a country-specific value set, where higher scores reflect better quality of life.
Both instruments have been validated for use in Indonesian populations in previous research, ensuring cultural and linguistic appropriateness. Reliability scores (Cronbach’s alpha) in prior studies were ≥ 0.8 (24, 25). Both the control and intervention groups completed a pre-intervention (baseline) assessment comprising demographic information, the MARS questionnaire, and the EQ-5D-5L. After one month, participants completed a post-intervention assessment using the same instruments. The data was managed using Microsoft Excel. Adherence and quality-of-life outcomes were evaluated by comparing pre- and post-test scores between groups.
Statistical Analysis
All statistical analyses were conducted using RStudio (version 2024.03, R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were first computed to summarize participant characteristics, adherence levels, and quality of life scores. Continuous variables were reported as means with standard deviations (SD), and categorical variables as frequencies with percentages.
To assess the effect of the TB-R mobile application, the Paired t-test was used to compare pre- and post-intervention scores (delta values) within each group for medication adherence and quality of life. This test was appropriate for detecting within-subject changes over time.
The Independent t-test was then employed to compare the mean differences in outcome changes (post-test minus pre-test values) between the intervention and control groups, enabling evaluation of the app’s effect across groups.
To explore the influence of demographic factors and interaction effects on adherence and quality of life, we applied Generalized Linear Models (GLM). These models allowed for the inclusion of multiple covariates (e.g., age, gender, employment, living status) and their interactions to assess their adjusted impact on outcome variables. The GLM was specified with a Gaussian family and identity link function for continuous outcomes. Model assumptions were tested and met. Statistical significance was defined as p < 0.05. Given the number of comparisons and interaction terms tested in the GLM, a Bonferroni correction was applied to control for the risk of Type I error. Adjusted p-values were used to determine statistical significance where applicable.
Results
Overview
The majority of patients were male (55.8%) and aged 40–50 years (43.0%), making them the most represented subgroup. Only a small proportion fell into the youngest (18–28 years, 16.3%) and oldest (> 60 years, 2.3%) age categories. This suggests that the majority of participants identified with one gender, with relatively balanced representation between the two groups. Most individuals were in the middle-aged age group, with a notable concentration observed in certain decades. Only a small proportion fell into the youngest and oldest age categories.
In terms of occupational engagement, a higher proportion reported active employment, while the remainder indicated otherwise. Regarding living arrangements, most participants reported residing with others, whereas a smaller group indicated living independently. The description of the characteristics of lung tuberculosis patients in this study can be seen in Table 1.
| Characteristics | Frequency | Percentage |
|---|---|---|
| Gender | ||
| Male | 48 | 55.8% |
| Female | 38 | 44.2% |
| Total | 86 | 100% |
| Age | ||
| 18-28 Years | 14 | 16.3% |
| 29-39 Years | 12 | 13.9% |
| 40-50 Years | 37 | 43.0% |
| 51-60 Years | 21 | 24.4% |
| Over 60 Years | 2 | 2.3% |
| Total | 86 | 100% |
| Employment Status | ||
| Work | 52 | 60.5% |
| Doesn't work | 34 | 39.5% |
| Total | 86 | 100% |
| Residence Status | ||
| Living Alone | 26 | 30% |
| Living together | 60 | 70% |
| Total | 86 | 100% |
Patient’s Medication Adherence
In the intervention group, adherence to anti-tuberculosis medication significantly improved following the implementation of the application. At baseline, 72.0% (n = 31) of participants in this group were adherent, increasing to 97.7% (n = 42) at end line. The reduction in non-adherent patients from 28.0% to 2.3% was statistically significant (p < 0.001). In contrast, the control group showed no meaningful change. Adherence was 76.7% (n = 33) at baseline and 79.0% (n = 34) at end line, with non-adherence rates shifting minimally from 23.3% to 21.0%. This difference was not statistically significant (p = 0.983).
When analyzed across both groups, overall adherence increased from 74.4% (n = 64) at baseline to 88.4% (n = 76) post-intervention, while non-adherence declined from 25.6% to 11.6%. These findings suggest a marked positive impact of the digital intervention on medication adherence among TB patients. Additionally, the effect size (Cohen’s d) for the improvement in adherence within the intervention group was calculated at 1.09, indicating a large effect size, while the between-group effect size was 0.84, suggesting a substantial difference due to the intervention. The 95% confidence interval for the change in adherence in the intervention group ranged from +15.1% to +32.5%, further supporting the robustness of the result.
Patient’s Quality of Life
Assessment of health-related quality of life using the EQ-5D-5L instrument revealed no cases of severe or extreme problems across any dimensions in both intervention and control groups at baseline or end line. In the intervention group, the highest proportion of patients reporting no problems (Level 1) at baseline was found in the Self-Care dimension (n = 34, 79.1%). The most frequently reported issue was moderate anxiety or depression (Level 3) in 18.6% of patients (n = 8). After one month of using the TB-R app, there was a marked increase in the proportion of patients reporting no problems across all dimensions and a corresponding reduction in reported health issues (Levels 2–5).
In the control group, the baseline dimension with the highest proportion of patients reporting no problems was Mobility (n = 32, 74.4%), while the most commonly reported issue was moderate difficulty in Self-Care (Level 3) affecting 23.3% of patients (n = 10). At the one-month follow-up, the number of patients reporting problems declined slightly across all dimensions, with a modest increase in those reporting no problems. The greatest improvement was observed in the Anxiety/Depression domain, increasing from 41.9% to 83.7% of patients reporting “no problems.” Self-Care and Usual Activities also showed gains above 15%. See Table 2 for detailed breakdown.
| Group | Level | Mobility [n (%)] | Self-Care [n (%)] | Usual activities [n (%)] | Pain / Discomfort [n (%)] | Anxiety / Depression [n (%)] | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | End Line | Baseline | End Line | Baseline | End Line | Baseline | End Line | Baseline | End Line | ||
| Test | No problems | 31 (72.1) | 40 (93.0) | 34 (79.1) | 41 (95.3) | 32 (74.4) | 42 (97.7) | 23 (53.5) | 39 (90.7) | 18 (41.9) | 36 (83.7) |
| Control | 32 (74.4) | 37 (86.0) | 30 (69.7) | 35 (81.4) | 30 (69.7) | 39 (90.7) | 28 (65.1) | 35 (81.4) | 21 (48.8) | 30 (69.7) | |
| Test | Slight problems | 7 (16.3) | 3 (7.0) | 7 (16.3) | 2 (4.7) | 9 (21.0) | 1 (2.3) | 15 (34.9) | 3 (4.0) | 17 (39.5) | 6 (14.0) |
| Control | 8 (18.6) | 6 (14.0) | 3 (7.0) | 8 (18.6) | 7 (16.3) | 4 (9.3) | 10 (23.3) | 6 (14.0) | 13 (30.2) | 10 (23.3) | |
| Test | Moderate problems | 5 (11.6) | 0 | 2 (4.6) | 0 | 2 (4.6) | 0 | 5 (11.6) | 1 (2.3) | 8 (18.6) | 1 (2.3) |
| Control | 3 (7.0) | 0 | 10 (23.3) | 0 | 6 (14.0) | 0 | 5 (11.6) | 2 (4.6) | 9 (21.0) | 3 (7.0) | |
| Test | Severe problems | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Control | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Test | Unable | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Control | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
Regarding overall quality of life, the proportion of patients in the intervention group reporting a "Good" quality of life increased from 72.0% at baseline (n = 31) to 93.0% at end line (n = 40), with the difference reaching statistical significance (p = 0.001). Meanwhile, the control group showed only a marginal improvement, from 74.4% to 79.0%, which was not statistically significant (p = 0.164). Across both groups, no participants reported a "Bad" quality of life at either time point. The mean EQ-5D index score in the intervention group increased from 0.81 ± 0.12 to 0.92 ± 0.06, with a mean difference of 0.11 (95% CI: 0.07 to 0.15, p < 0.01), indicating a statistically significant improvement. The control group only saw a non-significant increase from 0.83 ± 0.10 to 0.85 ± 0.09, with a mean difference of 0.02 (p = 0.11).
Impact of Patient Demographics on Medication Adherence and Quality of Life
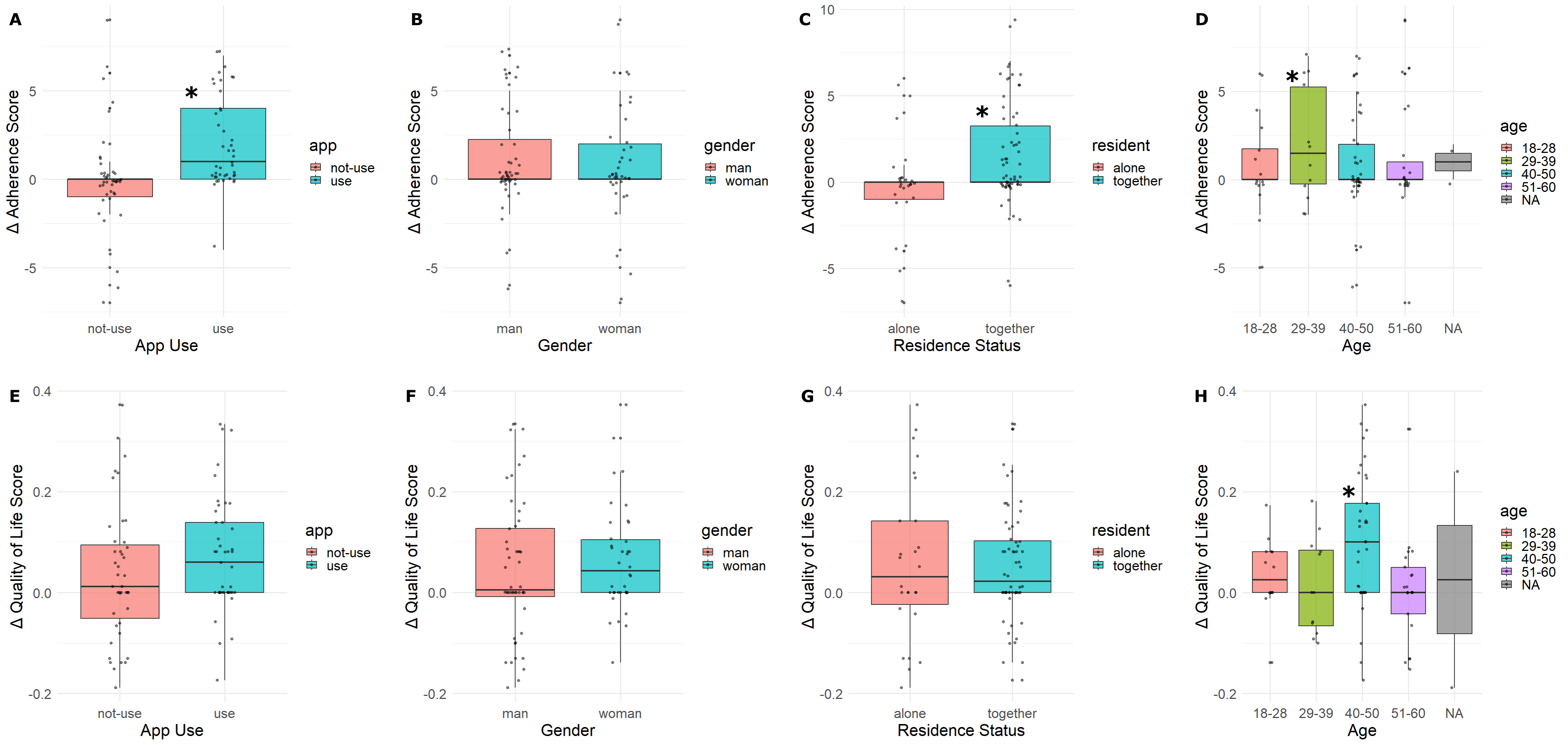
Based on the independent t-test analysis using delta values (post-test minus pre-test), the use of the TB-R application significantly improved patient medication adherence (p < 0.05). However, no statistically significant improvement was observed in patients’ quality of life.
Patients who lived with family demonstrated better adherence compared to those living alone, regardless of whether they used the TB-R app. In terms of age, patients aged 29–39 showed a significant improvement in medication adherence, while those aged 40–50 experienced a significant improvement in quality of life. These effects appeared to be independent of app usage and may be associated with increased age-related awareness or motivation to maintain health through regular physical activity. No significant effects were found for gender or employment status in relation to either medication adherence or quality of life.
As shown in Figure 1 and Table 2, the TB-R group exhibited consistent improvements across all five EQ-5D dimensions, particularly in Anxiety/Depression and Self-Care domains, suggesting psychological reassurance and enhanced self-management. Table 2 clearly illustrates the shift from moderate/slight issues to “no problems” across dimensions post-intervention.
Relationship Between Variables and Their Impact on Patient Medication Adherence and Quality of Life
The study also explored interactions between demographic variables and their combined effects on adherence and quality of life. Employed individuals who used the TB-R app showed improvement in both adherence and quality of life, although the result did not reach statistical significance (p = 0.06) (see Figure 2).
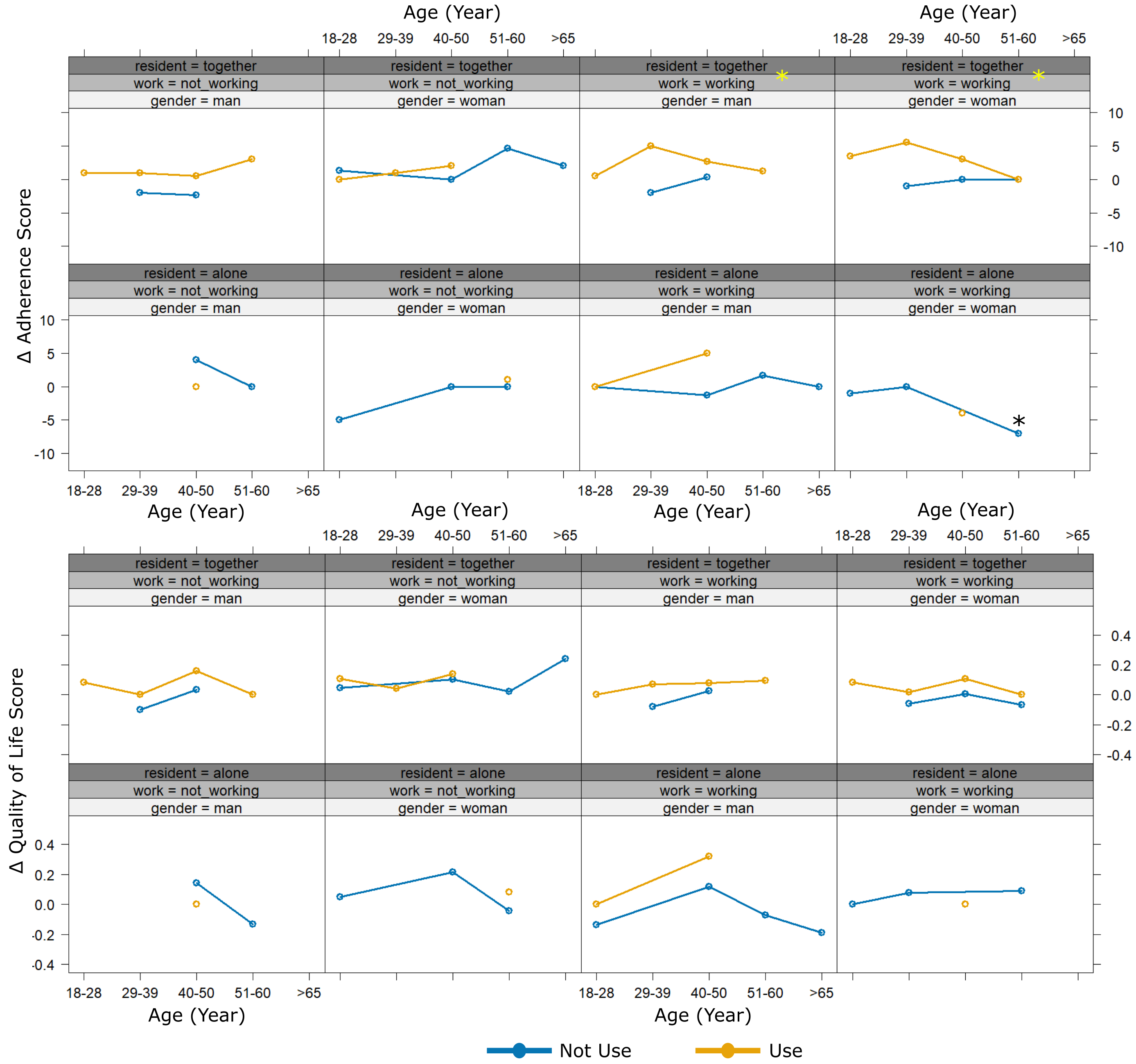
Furthermore, patients who were both employed and lived with others demonstrated a statistically significant increase in medication adherence (p < 0.05). In contrast, women aged 51–60 who lived alone showed a significant decline in medication adherence (p < 0.05). Interestingly, patients within this age range, both men and women, living alone or not, experienced a significant improvement in quality of life following the use of the TB-R application.
Discussion
Improving medication adherence is critical to the success of TB treatment. Non-adherence can compromise therapeutic outcomes, contribute to drug resistance, increase health system costs, and reduce patients’ overall quality of life (26-28). There is growing evidence in the Indonesian context that adherence is closely linked to quality of life outcomes among TB patients, suggesting that enhanced compliance can translate into measurable improvements in patient well-being (29-31).
This study demonstrates that the TB-R mobile application significantly improved medication adherence in the intervention group. These findings are in line with global literature emphasizing the importance of interactive digital tools for adherence management. A recent meta-analysis by Kim et al. (2023) concluded that mobile applications with reminder and feedback components achieved higher adherence gains than simple SMS systems, with pooled odds ratios of 2.15 across randomized controlled trials (32). Furthermore, this findings are consistent with previous research showing that digital tools, particularly SMS reminders, can positively influence TB medication adherence (33-35). Studies that integrated SMS with Video Directly Observed Therapy (VDOT) also reported similar improvements in adherence (36). However, some studies using SMS alone found no significant difference in adherence between intervention and control groups (22-23), suggesting that the effectiveness of such tools may depend on their design and level of user engagement. One noted limitation of SMS-based interventions is the inability to verify whether messages were actually read by patients (33). In contrast, the TB-R application used in this study incorporated a more interactive system, including repeated alarm notifications and user confirmation mechanisms. If a patient did not confirm medication intake, the notification would repeat, providing a persistent and personalized prompt. Unlike many SMS-only or passive reminder apps, TB-R prompts active user input and records behavioral responses, allowing real-time tracking and reinforcing adherence through feedback loops—features shown to be more effective in sustaining behavioral change in chronic disease management (15, 39). This enhanced feedback loop may explain the superior adherence outcomes observed. Furthermore, a systematic review by Jerene et al. (2023) found that the integration of behavioral nudges into mHealth applications substantially reduced treatment default rates, especially when apps were personalized and reinforced with local language and cultural adaptations (32).
Comparable tools, such as the TB-TST application trialed in Argentina, have also received positive feedback from users due to similar reminder features (24-25). In Indonesia, several pilot studies have explored mobile applications as adherence tools for TB patients (42-44), but few have rigorously evaluated their direct impact. A study by Fahdi et al. (2024) evaluated the “Mepet” application in Pontianak and reported that digital reminders improved treatment adherence among TB patients through a structured monitoring system (45). Similarly, Afriansyah et al. (2023) demonstrated the potential of the Android-based TB Re-Tuberis application to facilitate education and adherence monitoring in Bangka Belitung (46). These findings highlight the significance of mobile health in the TB care landscape in Indonesia, while also demonstrating that the interactive confirmation mechanism and real-time feedback provided by TB-R offer new advantages over static digital systems. Our findings contribute meaningful evidence to this gap, particularly in highlighting the importance of real-time feedback and behavioral reinforcement.
Notably, the TB-R application also led to improvements in quality of life, especially in the intervention group. Significant gains were observed across EQ-5D-5L dimensions, particularly in anxiety/depression and self-care. Although the overall change in quality of life did not reach statistical significance when comparing pre- and post-intervention scores directly, the direction and consistency of the improvements support the notion that enhanced adherence contributes to better patient-reported outcomes. The absence of severe or extreme problems across all EQ-5D-5L domains at both time points suggests that the sample population was relatively stable, making the observed changes even more noteworthy (47). The increase in the proportion of patients reporting a "Good" quality of life aligns with the substantial rise in adherence, suggesting that digital interventions may indirectly enhance well-being through improved treatment consistency and psychological reassurance. This increase in adherence was associated with favorable trends in quality of life across multiple domains, particularly in anxiety/depression and self-care. These patterns are consistent with previous findings indicating that improved adherence leads to better perceived health status and emotional stability among TB patients (48). In contrast, the control group, which received standard care without app-based support, showed only marginal changes, underscoring the added value of behavioral technology in TB management. These outcomes reflect WHO’s position on the use of digital adherence technologies (DATs), which are now strongly recommended for TB management in resource-limited settings, particularly for reinforcing patient engagement and psychological well-being (49).
This study also examined the influence of demographic factors. Living with others was associated with better adherence, regardless of app use, emphasizing the role of social support in chronic disease care. Family members can provide practical and emotional assistance, from medication reminders to moral encouragement, which is especially critical in settings where treatment regimens are prolonged and demanding (50). In contrast, patients living alone had lower adherence, likely due to reduced accountability and lack of reinforcement. This observation is consistent with findings by Gurusinga et al. (2024), who showed that familial support improves both treatment completion rates and emotional resilience among TB patients in Indonesian rural contexts (51).
Age-specific patterns emerged as well. Patients aged 29–39 showed significant adherence improvements, potentially due to higher digital engagement, regular routines, and increased health consciousness during early adulthood. Conversely, those aged 40–50 demonstrated notable improvements in quality of life, possibly reflecting greater psychological maturity, lifestyle changes, or intrinsic motivation toward wellness (52). These improvements appeared to occur independently of app use, indicating that personal and age-related factors can also play a key role in shaping outcomes. This aligns with research from China by Liu et al. (2023), which found that younger and tech-literate TB patients were more likely to engage consistently with app-based therapy support tools, resulting in higher medication adherence over time (53).
Gender and employment status alone did not show significant effects, but their interactions with other variables revealed important dynamics. Employed individuals using the TB-R app showed positive trends in both adherence and quality of life, albeit not statistically significant. Employment may provide a structured routine, purpose, and motivation, which, when combined with technological support, facilitates better self-management.
Of particular interest was the finding that patients who were both employed and lived with others experienced a significant increase in adherence, suggesting a synergistic effect of social and occupational structure. On the other hand, women aged 51–60 living alone exhibited a significant decline in adherence. This subgroup may face unique barriers, including lower social support, caregiving stress, health-related challenges, or discomfort with technology (54). Possible contributing factors include limited digital literacy and motivational fatigue, both of which have been reported as adherence barriers in older female patients (55). Future interventions could explore voice-based reminders, simplified app navigation, or family-integrated alerts to accommodate users with low tech familiarity. These obstacles may hinder engagement with the app and adherence more broadly. In particular, digital literacy may be a contributing factor, as prior studies have shown that older women are less likely to engage with mobile health tools without prior exposure or guidance (55, 56). Additionally, motivational decline due to treatment fatigue and a lack of immediate social reinforcement may have compounded the adherence gap in this group. Nevertheless, the same age group showed significant gains in quality of life, possibly due to improvements in emotional regulation, mood, or a sense of empowerment from even minimal engagement with health technology. This dual influence echoes the social-ecological framework, where individual behavior is enhanced by workplace structure and social reinforcement—factors often leveraged in successful chronic disease management strategies (57). Additionally, future interventions could explore incorporating family-based support systems, even remotely, and adapting app features to include voice-based instructions or automated audio reminders tailored to users with digital disabilities. Integrating community health workers or peer supporters may also increase motivation and accountability. These strategies have shown promise in similar settings where digital access is limited or underutilized (53).
Recommendation and Future Research
Taken together, the findings affirm that digital adherence tools like TB-R can be powerful adjuncts to TB treatment, but their effectiveness is shaped by demographic context. A one-size-fits-all approach may not be sufficient. Tailored strategies that consider living arrangements, age, employment, and gender-specific barriers are essential to maximizing impact. Future research should focus on longitudinal outcomes to assess sustained adherence and clinical effectiveness. Incorporating qualitative feedback could provide deeper insight into user experiences, while implementation studies can identify how best to scale and integrate digital tools within national TB programs. Special attention should be given to vulnerable subgroups, such as older adults living alone, who may require additional support beyond digital interventions to achieve optimal treatment outcomes.
Conclusion
The TB-R application showed a statistically significant improvement in medication adherence among pulmonary tuberculosis patients and a modest, improvement in certain dimensions of quality of life,, with benefits that did not consistently reach statistical significance across all domains. The intervention's impact appeared to be enhanced when supported by social and demographic factors such as age, living situation, and employment. These findings highlight the potential of digital tools to enhance TB treatment outcomes, particularly in supporting medication adherence, but also underscore the need for tailored interventions that address individual patient contexts. However, conclusions regarding quality of life improvements should be interpreted with caution due to the short duration of the study and limited statistical significance in some domains. Future research with longer follow-up periods, larger sample sizes, and multicenter designs is needed to validate the sustainability and generalizability of the TB-R application's effects. Integrating technology with social support strategies may offer the most effective path to improving adherence and overall patient well-being.
Declarations
Acknowledgment
The researcher would like to thank the Directorate of Research, Technology, and Community Service, Ministry of Education and Culture, Research and Technology of the Republic of Indonesia for providing funding for this research through the 2024 Fiscal Year Research Program Grant with research contract number 130/SP2H/RT-MONO/LL4/2024.
Conflict of Interest
The authors declare no conflicting interest.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to confidentiality agreements with participating institutions and privacy considerations of patient data. However, anonymized data may be made available from the corresponding author upon reasonable request and with permission from the relevant ethics committee.
Ethics Statement
This study has gone through an ethical review from the Health Research Ethics Commission of Respati University of Yogyakarta with the number 110.3/FIKER/PL/VIII/2024 on August 12, 2024.
Funding Information
This research was supported by Directorate of Research, Technology, and Community Service, Ministry of Education and Culture, Research and Technology of the Republic of Indonesia, under grant number 130/SP2H/RT-MONO/LL4/2024. The funding organization had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- Suarnianti, Safitri R, Ratna. Health Literacy Meningkatkan Quality Of Life (QoL) Penderita Tuberkulosis Paru. Healthc Nurs J. 2022;4(2):342–8.
- Kementerian Kesehatan RI. Profil kesehatan Indonesa 2019 [Internet]. Kementerian Kesehatan Republik Indonesia. Jakarta: Kementerian Kesehatan RI; 2020. 487 p. Available from: https://pusdatin.kemkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/Profil-Kesehatan-indonesia-2019.pdf
- Ghazy R, Ashmawy R, Reyad O, Abd ElHafeez S, El-Shishtawy M, Khedr H, et al. Translation and cultural adaptation of the WHO generic tuberculosis patient cost survey to an Egyptian context. East Mediterr Health J. 2022;28(9):649–57.
- Kementerian Kesehatan RI. Strategi Nasional Penanggulangan Tuberkulosis di Indonesia 2020-2024. Kementeri Kesehat RI. 2020;135.
- Adhanty S, Syarif S. Kepatuhan Pengobatan pada Pasien Tuberkulosis dan Faktor-Faktor yang Mempengaruhinya: Tinjauan Sistematis. J Epidemiol Kesehat Indones. 2023;7(1):7-14.
- Pomalango ZB, Arsyad SFM. Hubungan Tingkat Pengetahuan tentang TB Resisten Obat (TB-RO) dengan Kepatuhan Minum Obat Pasien TB Paru. Jambura Nurisng J. 2024;6(1):92–104.
- The Ministry of Health Republic of Indonesia. Revised National Strategy of Tuberculosis Care and Prevention in Indonesia 2020-2024 and Interim Plan for 2025-2026. 2023.
- Hayatinufus MPP, Suwendar, Fitrianingsih SP. Studi Analisis Tingkat Kepatuhan Terapi pada Pasien TB Paru Dewasa di Poli TB UPT Puskesmas Pasundan Kota Bandung. Bandung Conf Ser Pharm. 2023;8:43–9.
- Miller R, Goodman C. Quality of tuberculosis care by pharmacies in low- and middle-income countries: Gaps and opportunities. J Clin Tuberc Other Mycobact Dis [Internet]. 2020;18:100135.
- Gao Z, Wang P, Hong J, Yan Y, Tong T, Wu B, et al. Health-related quality of life among Chinese patients with Crohn’s disease: a cross-sectional survey using the EQ-5D-5L. Health Qual Life Outcomes [Internet]. 2022;20(1):1–9.
- Aggarwal AN. Quality of life with tuberculosis. J Clin Tuberc Other Mycobact Dis [Internet]. 2019;17:100121.
- Ita W, Yusran S, Sety LOM. Gambaran Kualitas Hidup Penderita TB Paru Di Wilayah Kerja Puskesmas Perumnas Kota Kendari Tahun 2019. Endem J. 2020;1(3):27–32.
- Alfauzan, Lucya V. Gambaran kualitas hidup pada penderita tuberkulosis di asia: Literature Review. J Keperawatan. 2021;7(3):65–70.
- Joe W, Rinju, Patel N, Alambusha R, Kulkarni B, Yadav K, et al. Coverage of iron and folic acid supplementation in India: Progress under the Anemia Mukt Bharat strategy 2017-20. Health Policy Plan. 2022;37(5):597–606.
- Lee S, Rajaguru V, Baek JS, Shin J, Park Y. Digital Health Interventions to Enhance Tuberculosis Treatment Adherence: Scoping Review. JMIR mHealth uHealth. 2023 Dec;11:e49741.
- Syahrul S, Irwan AM, Saleh A, Syam Y, Fiqri AM, Jannah SN. Effectiveness of Mobile Application-Based Intervention on Medication Adherence Among Pulmonary Tuberculosis Patients: A Systematic Review. Comput Inform Nurs. 2025 Apr;43(4): e01213.
- Nglazi MD, Bekker L-G, Wood R, Hussey GD, Wiysonge CS. Mobile phone text messaging for promoting adherence to anti-tuberculosis treatment: a systematic review protocol. Syst Rev. 2013 Jan;2:566.
- Ridho A, Alfian SD, van Boven JFM, Levita J, Yalcin EA, Le L, et al. Digital Health Technologies to Improve Medication Adherence and Treatment Outcomes in Patients With Tuberculosis: Systematic Review of Randomized Controlled Trials. J Med Internet Res. 2022 Feb;24(2):e33062.
- Asosiasi Penyelenggara Jasa Internet Indonesia. Penetrasi dan Profil Perilaku Pengguna Internet Indonesia [Internet]. 2023 [cited 2024 Mar 5]. Available from: https://survei.apjii.or.id/home
- Sari P, Herawati DMD, Dhamayanti M, Ma’ruf TLH, Hilmanto D. The Effect of Mobile Health (m-Health) Education Based on WANTER Application on Knowledge, Attitude, and Practice (KAP) Regarding Anemia among Female Students in a Rural Area of Indonesia. Healthc. 2022;10(10):1993.
- Tanberika FS, Sansuwito T Bin, Hassan HC. Effectiveness Of Android Based Antenatal Care Application To Enhance Antenatal Care Adherence And Pregnant Mothers Health: A Literature Review. Int J Heal Sci. 2023;1(2):37–44.
- Zaman C, Priyatno AD, Zetira NR. Kepatuhan Pasien Rawat Jalan Poli Paru Dalam Penggunaan Obat Anti Tuberkulosis (Oat) Di Rumah Sakit Kartika Husada Jatiasih Bekasi. MALAHAYATI Heal STUDENT J. 2023;3(12):3849–3870.
- Halim M, Sabrina A, Aris M. Kepatuhan Pasien Rawat Jalan Poli Paru Dalam Penggunaan Obat Anti Tuberkulosis (Oat) Di Rumah Sakit Kartika Husada Jatiasih Bekasi. Jurnal Farmasi IKIFA. 2023;5(1):1–14.
- Tondok SB, Watu E, Wahyuni W. Validitas instrumen European Qualitiy of Life (EQ-5D-5L) Versi Indonesia untuk menilai kualitas hidup penderita tuberkulosis. Holistik J Kesehat. 2021;15(2):267–73.
- Octavia DR, Sholikha J, Utami PR. Uji Validitas dan Reliabilitas Kuesioner Medication Adherence Report Scale ( MARS ) terhadap Pasien Tuberkulosis ( TB ) Validity and Reliability Test of the Medication Adherence Report Scale ( MARS ) Questionnaire for Tuberculosis ( TB ) Patients. J Pharm Sci. 2024;9(1):7–10.
- Lutfian L, Azizah A, Wardika IJ, Wildana F, Maulana S, Wartakusumah R. The role of family support in medication adherence and quality of life among tuberculosis patients: A scoping review. Japan J Nurs Sci. 2025;22(1):1–11.
- Kastien-Hilka T, Rosenkranz B, Schwenkglenks M, Bennett BM, Sinanovic E. Association between health-related quality of life and medication adherence in pulmonary tuberculosis in South Africa. Front Pharmacol. 2017;8:919.
- Yadav RK, Kaphle HP, Yadav DK, Marahatta SB, Shah NP, Baral S, et al. Health related quality of life and associated factors with medication adherence among tuberculosis patients in selected districts of Gandaki Province of Nepal. J Clin Tuberc Other Mycobact Dis [Internet]. 2021;23:100235.
- Nurhayati A, Rahayuningsih N, Alifiar I. Analisis Kualitas Hidup (QoLY) Dan Kepatuhan Terapi Pada Pasien Tuberkulosis Paru Di Rumah Sakit X Kota Tasikmalaya. Anal Kualitas Hidup … J Pharmacopolium. 2020;3(3):183–189.
- Maimunah R, Ardiyantoro B. Analisis hubungan tingkat kepatuhan pengobatan pasien tuberkulosis dengan kualitas hidup pasien di puskesmas ngemplak. 2024;5:10156–10164.
- Papeo DRP, Immaculata M, Rukmawati I. Hubungan Antara Kepatuhan Minum Obat (MMAS-8) Dan Kualitas Hidup (WHOQOL-BREF) Penderita Tuberkulosis Di Puskesmas Di Kota Bandung. Indones J Pharm Educ. 2021;1(2):86–97.
- Jerene D, Levy J, Van Kalmthout K, Rest J Van, McQuaid CF, Quaife M, et al. Effectiveness of digital adherence technologies in improving tuberculosis treatment outcomes in four countries: a pragmatic cluster randomised trial protocol. BMJ Open. 2023;13(3):e068685.
- Badzi CD, Kotoh AM, Tabong PT-N, Maya ET, Torpey K, Kwara A, et al. SMS reminders for monitoring tuberculosis treatment among women in Greater Accra region, Ghana. Digit Heal [Internet]. 2024;10:20552076241297744.
- Fang XH, Guan SY, Tang L, Tao FB, Zou Z, Wang JX, et al. Effect of short message service on management of pulmonary tuberculosis patients in Anhui Province, China: A prospective, randomized, controlled study. Med Sci Monit. 2017;23:2465–2469.
- Albino S, Tabb KM, Requena D, Egoavil M, Pineros-Leano MF, Zunt JR, et al. Perceptions and acceptability of short message services technology to improve treatment adherence amongst tuberculosis patients in Peru: A focus group study. PLoS One. 2014;9(5):1–6.
- Hoffman JA, Cunningham JR, Suleh AJ, Sundsmo A, Dekker D, Vago F, et al. Mobile Direct Observation Treatment for Tuberculosis Patients. A Technical Feasibility Pilot Using Mobile Phones in Nairobi, Kenya. Am J Prev Med. 2010;39(1):78–80.
- Mohammed S, Glennerster R, Khan AJ. Impact of a daily SMS medication reminder system on tuberculosis treatment outcomes: A randomized controlled trial. PLoS One. 2016;11(11):1–13.
- Bediang G, Stoll B, Elia N, Abena JL, Geissbuhler A. SMS reminders to improve adherence and cure of tuberculosis patients in Cameroon (TB-SMS Cameroon): A randomised controlled trial. BMC Public Health. 2018;18(1):1–15.
- Thakkar J, Kurup R, Laba T-L, Santo K, Thiagalingam A, Rodgers A, et al. Mobile Telephone Text Messaging for Medication Adherence in Chronic Disease: A Meta-analysis. JAMA Intern Med. 2016 Mar;176(3):340–349.
- Iribarren S, Milligan H, Goodwin K, Vidrio OAA, Chirico C, Telles H, et al. Mobile tuberculosis treatment support tools to increase treatment success in patients with tuberculosis in argentina: Protocol for a randomized controlled trial. JMIR Res Protoc. 2021;10(6):e28094.
- Iribarren SJ, Milligan H, Chirico C, Goodwin K, Schnall R, Telles H, et al. Patient-centered mobile tuberculosis treatment support tools (TB-TSTs) to improve treatment adherence: A pilot randomized controlled trial exploring feasibility, acceptability and refinement needs. Lancet Reg Heal - Am [Internet]. 2022;13:100291.
- Gunadi G, Widjanarko B, Shaluhiyah Z. Pengembangan Aplikasi “Kang Tb” Untuk Pengawas Menelan Obat Pasien Tuberkulosis Di Kabupaten Pekalongan. Jambura J Heal Sci Res. 2023;5(3):964–977.
- Kusumawati K. Aplikasi Monitoring Pasien Tuberkulosis di Puskesmas Kebayoran Lama. J Manaj Inform. 2023;13(2):135–147.
- Reyaan IBM, Faustincia I, Zazuli Z. Dampak Intervensi Edukasi dan Aplikasi Pengingat Minum Obat terhadap Pengetahuan dan Kepatuhan Pasien Tuberkulosis Paru di Puskesmas di Kota Bandung. J Manaj Dan Pelayanan Farm (Journal Manag Pharm Pract. 2023;13(4):256–265.
- Fahdi F, Novianry V, Sastriawan H. Pengaruh Aplikasi Mepet Terhadap Kepatuhan Minum Obat Pada Pasien Tubercolosis. J Keperawatan dan Kesehat [Internet]. 2024 Apr 30;15(1 SE-Articles).
- Afriansyah R, Lanaya D, Sari L, Azrul M, Riyad M. Perancangan Aplikasi Re-Tuberis (Remember Tuberculosis) Dalam Pelayanan Informasi Dan Kepatuhan Penggunaan Obat. J Manaj Inf Kesehat Indones. 2023;11(2):157–164.
- Kangwanrattanakul K. Normative profile of the EQ-5D-5L dimensions, EQ-5D-5L index and EQ-VAS scores for the general Thai population. Qual Life Res. 2023 Sep;32(9):2489–2502.
- Sinaga BYM, Az Zahra DA, Simatupang MM, Wahyuni AS. Factors Associated with Quality of Life among Pulmonary Tuberculosis Patients. Univers J Public Heal. 2024;12(2):315–325.
- World Organization for Animal Health. Report 20-23. Vol. t/malaria/, January. 2023.
- Wahlund L-O, Winblad B. Dementia: diagnostics, early treatment, and assistance from family members. Acta Neurol Scand. 1996 Dec;94:2–22.
- Gurusinga R, Bachtiar A, Machmud R, Burhan E, Semiarty R. Family Support Pattern For Treatment Adherence Among Tuberculosis Patients In Deli Serdang Regency : 2024;(July):220–233.
- Brothers A, Gabrian M, Wahl H-W, Diehl M. Future time perspective and awareness of age-related change: Examining their role in predicting psychological well-being. Psychol Aging. 2016 Sep;31(6):605–617.
- Liu X, Thompson J, Dong H, Sweeney S, Li X, Yuan Y, et al. Digital adherence technologies to improve tuberculosis treatment outcomes in China: a cluster-randomised superiority trial. Lancet Glob Heal. 2023 May;11(5):e693–703.
- Reynolds CF, Jeste D V., Sachdev PS, Blazer DG. Mental health care for older adults: recent advances and new directions in clinical practice and research. World Psychiatry. 2022 Oct;21(3):336–363.
- Borges do Nascimento IJ, Abdulazeem H, Vasanthan LT, Martinez EZ, Zucoloto ML, Østengaard L, et al. Barriers and facilitators to utilizing digital health technologies by healthcare professionals. npj Digit Med. 2023;6(1):1–28.
- Aisyah DN, Ahmad RA, Artama WT, Adisasmito W, Diva H, Hayward AC, et al. Knowledge, Attitudes, and Behaviors on Utilizing Mobile Health Technology for TB in Indonesia: A Qualitative Pilot Study. Front Public Heal. 2020;8(October):1–9.
- Nguyen KH, Cemballi AG, Fields JD, Brown W, Pantell MS, Lyles CR. Applying a socioecological framework to chronic disease management: Implications for social informatics interventions in safety-net healthcare settings. JAMIA Open. 2022;5(1):1–10.